
High-throughput drug screening is defined as an automated method for testing large chemical or biological compound libraries to identify active molecules in drug discovery. A campaign qualifies as high-throughput if it runs over 10,000 assays per day; ultra-high-throughput screening (uHTS) reaches up to 100,000 assays per day. That scale compresses years of manual testing into weeks. The method rests on four foundational stages: library preparation, assay development, automation via robotic platforms, and data analysis for hit identification. Researchers who understand each stage design better campaigns and interpret results with far greater confidence.
What is high-throughput drug screening and how does it work?
High-throughput drug screening (HTS) is the systematic, automated evaluation of thousands to millions of compounds against a biological target. The goal is to identify "hits," compounds that show measurable activity and warrant further investigation as potential drug candidates. HTS sits at the front end of the drug discovery pipeline, feeding lead optimization and preclinical development with validated starting points.
The four-stage HTS process moves from compound library preparation through assay development, robotic execution, and computational data analysis. Each stage depends on the one before it. A poorly prepared library or an under-validated assay will corrupt results regardless of how sophisticated the automation is.

HTS is not simply fast testing. The method requires miniaturized assay formats, typically 384-well or 1,536-well plates, to increase throughput while reducing reagent consumption. Miniaturization also reduces cost per data point, which matters when screening libraries of hundreds of thousands of compounds. The types of FDA-approved drug screens used in clinical and research contexts share this emphasis on standardization and reproducibility.
What are the key stages of the high-throughput screening process?
The full HTS workflow spans nine distinct steps, each with defined quality gates before advancing to the next.
- Target biology selection. Define the biological target, its mechanism, and the disease relevance. A poorly chosen target wastes every downstream resource.
- Assay format definition. Choose between biochemical or cell-based formats based on target biology and available reagents.
- Assay optimization. Titrate reagent concentrations, incubation times, and detection conditions to maximize signal quality.
- Assay validation. Confirm reproducibility, signal stability, and suitability for automation using quality metrics such as the Z-prime factor.
- Miniaturization. Transfer the validated assay from standard 96-well plates to 384-well or 1,536-well formats to increase throughput.
- Automation integration. Program liquid handling robots and automated readers to execute the assay without manual intervention.
- Pilot screening. Run 1–5% of the compound library to identify automation or reagent stability issues before committing to full scale.
- Full-scale screening. Execute the complete library screen under controlled, automated conditions.
- Hit triage. Apply predefined criteria to rank and filter active compounds for follow-up confirmation assays.
Each step requires documentation and sign-off. Skipping validation or miniaturization to save time creates compounding errors that surface only after full-scale screening, at far greater cost.
What types of assays are used in high-throughput screening?
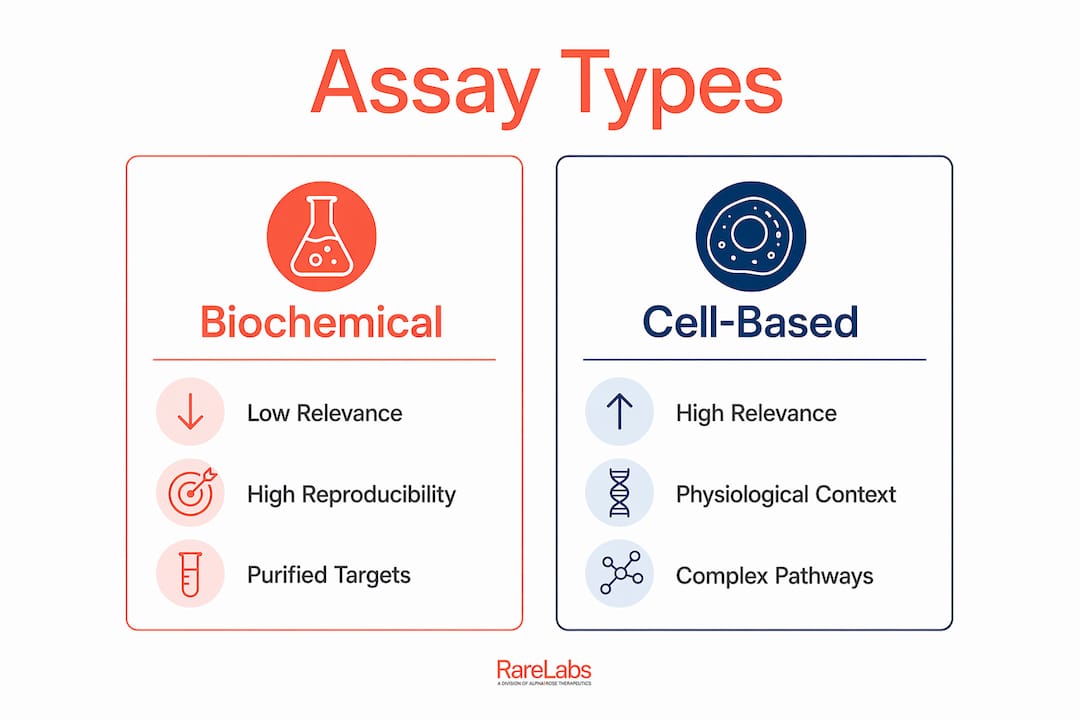
Assay format is one of the most consequential decisions in any HTS campaign. The two primary categories are biochemical assays and cell-based assays, and they serve different scientific purposes.
| Assay type | Biological relevance | Reproducibility | Best suited for |
|---|---|---|---|
| Biochemical | Low to moderate | High | Direct enzyme or receptor binding studies |
| Cell-based | High | Moderate | Pathway activity, phenotypic readouts |
| Phenotypic | Very high | Lower | Disease-relevant cellular models |
Biochemical assays measure direct molecular interactions between a compound and a purified target protein. They deliver high reproducibility and clean signal-to-noise ratios, making them well suited for target-focused campaigns. The trade-off is that they do not capture cellular context, membrane permeability, or off-target effects.
Cell-based assays measure compound activity within living cells, capturing pathway complexity and physiological relevance that biochemical formats miss. They are harder to miniaturize and more sensitive to environmental variability, but they produce hits with stronger translational potential. Hopeatrarelabs uses patient-derived cell models, including induced pluripotent stem cells (iPSCs), to bring disease-relevant biology directly into the screening process.
Detection methods across both formats include fluorescence intensity, fluorescence polarization, time-resolved FRET, luminescence, and absorbance. Fluorescence-based methods dominate HTS because they are sensitive, non-destructive, and compatible with high-density plate formats. The choice of detection method affects assay sensitivity, compound interference risk, and instrument requirements.
What are best practices for designing robust assays for HTS?
Early assay development decisions dictate data quality, false positive rates, and the cost of follow-up work. Researchers who treat assay design as a formality pay for it during hit triage.
Key quality and risk factors to address before scaling:
- Z-prime factor validation. The Z-prime factor is the industry gold standard for assay quality, combining signal dynamic range and variability into a single metric. A Z-prime above 0.5 is the accepted threshold for proceeding to full-scale screening.
- Operator independence. Assay robustness requires workflows that produce consistent results regardless of who runs them. Any step that depends on individual technique introduces variability that compounds across thousands of wells.
- Reagent stability. Proteins, cell lines, and detection reagents degrade over time and across freeze-thaw cycles. Stability testing under actual screening conditions, not just bench conditions, is mandatory.
- Data normalization. Standardized normalization protocols correct for plate-to-plate variability and edge effects, which are systematic artifacts that appear in the outer wells of high-density plates.
- False positive mitigation. Fluorescent compounds, aggregators, and reactive molecules generate false signals. Counter-screens and orthogonal assay formats catch these before they consume follow-up resources.
Pro Tip: Design your hit triage criteria before you run a single compound. Knowing exactly what a "hit" means, activity threshold, selectivity requirement, and acceptable cytotoxicity, prevents post-hoc rationalization that inflates your hit list and wastes confirmation capacity.
The steps in custom ASO development follow a similar logic: decisions made at the design stage determine whether the downstream work succeeds or fails. The same principle applies to HTS assay design.
How does automation drive efficiency in high-throughput screening?
Automation is what separates HTS from conventional screening. Without robotic platforms, the throughput numbers that define HTS are physically impossible to achieve. The core components of an automated HTS system include:
- Liquid handling robots. These dispense nanoliter to microliter volumes of compounds and reagents with precision that no human pipetting can match at scale. They also eliminate the repetitive motion errors that accumulate over long manual runs.
- Automated incubators and plate stackers. These maintain controlled environmental conditions and feed plates to instruments in sequence, enabling continuous, unattended operation.
- Automated plate readers. Fluorescence, luminescence, and absorbance readers capture data from every well in seconds. High-content imaging systems add morphological readouts to standard intensity measurements.
- Laboratory information management systems (LIMS). Software captures raw data, applies normalization algorithms, flags outliers, and ranks hits against predefined thresholds. Without integrated data management, the data volume generated by HTS campaigns becomes unmanageable.
The automation advancements driving biopharma productivity in 2026 include AI-assisted hit prioritization and real-time quality monitoring that flags plate failures during a run rather than after. These capabilities reduce wasted screening cycles and improve the signal-to-noise ratio of the final hit list. The practical result is that researchers spend less time troubleshooting data and more time evaluating genuine candidates.
What practical considerations shape a successful HTS campaign?
Successful HTS campaigns share one characteristic: the team planned for failure before it happened. Pilot screening 1–5% of the compound library before full-scale execution is the single most effective risk reduction step available. A pilot screen reveals automation timing issues, reagent degradation patterns, and plate-to-plate variability that small-scale validation tests never expose.
Hit triage planning is equally non-negotiable. Hit quality depends on clear downstream evaluation criteria defined before screening begins, not after. Teams that define activity thresholds, selectivity requirements, and acceptable physicochemical properties in advance produce hit lists that move efficiently into lead optimization. Teams that define criteria post-hoc produce hit lists that stall.
HTS also integrates with adjacent technologies to accelerate the full discovery timeline. Drug repurposing strategies use HTS to rapidly test approved compounds against new targets, compressing timelines by years. In rare disease research, this approach is particularly valuable because the patient populations are too small to support traditional discovery timelines. Hopeatrarelabs applies parallel treatment screens across thousands of FDA-approved drugs and custom antisense oligonucleotides (ASOs) to find viable options for patients with ultra-rare and undiagnosed genetic diseases.
Pro Tip: Run your pilot screen on a representative subset of the library, not just the easiest compounds to handle. Include known actives, known inactives, and structurally diverse compounds to stress-test the assay under realistic conditions.
Key Takeaways
High-throughput drug screening succeeds when assay design, automation, and hit triage criteria are all defined before full-scale screening begins.
| Point | Details |
|---|---|
| HTS throughput threshold | A campaign qualifies as HTS at over 10,000 assays per day; uHTS reaches 100,000 per day. |
| Assay format choice | Biochemical assays offer high reproducibility; cell-based assays deliver greater biological relevance. |
| Z-prime factor | A Z-prime above 0.5 is the accepted standard for assay quality before scaling to full campaigns. |
| Pilot screen value | Running 1–5% of the library before full-scale screening catches automation and reagent issues early. |
| Hit triage planning | Defining hit criteria before screening begins directly determines the quality of the final candidate list. |
Why assay design matters more than detection technology
Researchers entering HTS for the first time almost always focus on the wrong thing. They spend weeks evaluating plate readers and fluorescence detection systems while treating assay design as a formality. That is a costly inversion of priorities.
The detection instrument is interchangeable. The assay design is not. Every choice made during assay development, from reagent selection to signal generation strategy to variability control, determines the quality of data you will get from every single compound in your library. A weak assay run on the best automation platform in the world still produces weak data.
What I have seen work consistently is treating assay development as a risk management exercise from day one. Map every failure mode before you miniaturize. Ask what happens if the reagent degrades on day three of a five-day screen. Ask what your Z-prime looks like at the edges of a 1,536-well plate, not just in the center. These questions feel premature early in development. They feel obvious after a failed campaign.
The pilot screen is where most teams recover from design oversights they did not know they had. Run it seriously, analyze it rigorously, and be willing to go back to assay development if the data tells you to. The cost of a two-week delay at the pilot stage is a fraction of the cost of a failed full-scale campaign.
— John
Hopeatrarelabs resources for drug screening research
Researchers working at the intersection of HTS and rare disease drug discovery need more than general methodology guidance. They need resources built around the specific challenges of ultra-rare targets, small patient populations, and the urgency that defines this field.

Hopeatrarelabs maintains a curated knowledge hub at RareLabs Knowledge designed for exactly this audience. The resource covers rare disease research, treatment screening approaches, and the science behind patient-specific disease modeling using iPSCs and CRISPR. For researchers applying HTS principles to genetic disease targets, it offers context that general drug discovery resources do not. The drug screening tips for biopharma researchers section is a practical starting point for teams building or refining their screening workflows.
FAQ
What is high-throughput drug screening?
High-throughput drug screening is an automated process that tests large compound libraries against a biological target to identify active molecules. A campaign qualifies as HTS when it runs more than 10,000 assays per day.
How does high-throughput screening differ from standard drug screening?
Standard drug screening tests compounds manually and in small numbers, while HTS uses robotic automation and miniaturized assay formats to test tens of thousands of compounds per day with consistent reproducibility.
What is the Z-prime factor in HTS assay validation?
The Z-prime factor is the industry gold standard metric for assay quality, combining signal dynamic range and variability into a single score. A Z-prime above 0.5 is required before advancing an assay to full-scale screening.
What are the main advantages of high-throughput screening in drug discovery?
HTS compresses compound evaluation timelines from years to weeks, reduces cost per data point through miniaturization, and generates statistically robust datasets that improve the quality of lead candidates entering optimization.
Why is a pilot screen important before full-scale HTS?
A pilot screen of 1–5% of the compound library reveals automation failures, reagent instability, and plate variability that small-scale validation tests do not expose, preventing those issues from corrupting the full campaign.