
Most families enter the world of rare disease treatment believing gene therapy is either a distant dream or a treatment only available to a lucky few in academic trials. The reality is far more nuanced. A single gene therapy infusion can, in some cases, permanently correct the root cause of a life-threatening condition. But understanding which patients qualify, what options actually exist, and how to navigate a system full of gatekeepers requires far more than a basic internet search. This guide breaks down everything you need to know, from how these therapies work to the practical steps that separate families who find answers from those who don't.
Table of Contents
- What is gene therapy and how does it work for rare diseases?
- Emerging personalized therapies: N-of-1 and latest advances
- FDA-approved gene therapies: Options, outcomes, and patient access
- Barriers and practical considerations for families
- Getting started: Practical steps for families seeking gene therapy
- Our perspective: What most families miss about gene therapy for rare diseases
- Explore further: Personalized rare disease solutions and expert support
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Gene therapy basics | Gene therapy uses advanced delivery methods like viral vectors and lipid nanoparticles to treat rare diseases at their root. |
| Personalized treatments | N-of-1 therapies are revolutionizing care for ultra-rare diseases by crafting custom solutions for individual patients. |
| FDA-approved options | Several gene therapies are now FDA-approved for rare diseases, with some available cost-free or through Medicaid models. |
| Access challenges | High costs, immune responses, and regulatory barriers often limit patient access to gene therapy solutions. |
| Practical steps | Early diagnosis, trial enrollment, and ongoing advocacy are essential for families seeking gene therapy for ultra-rare diseases. |
What is gene therapy and how does it work for rare diseases?
Gene therapy is not one treatment. It is a category of approaches that share a common goal: fix the problem at the genetic level rather than manage symptoms indefinitely. Depending on the disease and the target tissue, the strategy and delivery method can look very different.
At the broadest level, gene therapy can:
- Replace a missing or broken gene with a functional copy
- Edit a gene directly using tools like CRISPR base editing or prime editing
- Modulate gene activity using antisense oligonucleotides (ASOs) that target RNA rather than DNA
In vivo therapies deliver the genetic payload directly into the patient's body, often via intravenous infusion. The vector, meaning the delivery vehicle, travels through the bloodstream and enters target cells. Ex vivo therapies remove cells from the patient, modify them in a lab setting, and reinfuse them. Both methods have distinct advantages depending on the tissue involved. You can read more about ex vivo gene therapy approaches and when they are most appropriate for rare disease cases.
The most widely used delivery system is the adeno-associated virus, or AAV. These are small, engineered viruses that carry genetic cargo without causing disease themselves. Different AAV serotypes (variants) have natural preferences for different tissues: AAV9 crosses the blood-brain barrier, making it ideal for neurological diseases like spinal muscular atrophy.
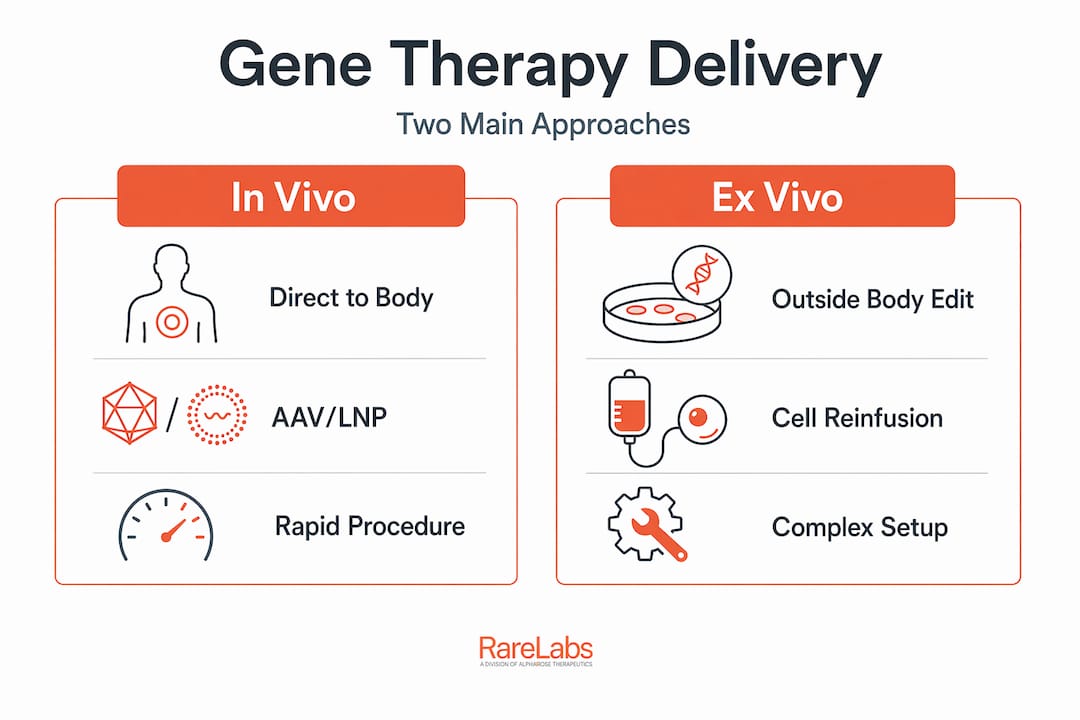
Emerging approaches for ultra-rare diseases use lipid nanoparticles (LNPs), which are tiny fat-based capsules that can carry mRNA or base editing components. LNPs avoid immune responses to viral vectors and can be manufactured faster, which matters enormously for one-of-a-kind therapies. Custom ASOs are another tool, directly silencing or modifying specific RNA transcripts without permanent DNA changes.
| Delivery approach | How it works | Best for | Key limitation |
|---|---|---|---|
| AAV (adeno-associated virus) | Viral vector; delivers DNA to target cells in vivo | Neurological, ocular, muscular diseases | Pre-existing anti-AAV immunity can disqualify patients |
| Lipid nanoparticle (LNP) | Fat capsule delivers mRNA or editing components | Liver-targeted or N-of-1 custom therapies | Transient expression; repeat dosing may be needed |
| Ex vivo cell modification | Patient cells edited outside the body, reinfused | Blood disorders (SCD, beta-thalassemia) | Requires conditioning regimen; complex logistics |
| Custom ASOs | RNA-targeting molecules block or redirect gene expression | Ultra-rare single-gene neurological diseases | Requires periodic dosing; patient-specific design |
Gene therapy primarily uses viral vectors like AAV for in vivo or ex vivo gene replacement, editing, or modulation in rare diseases. Understanding this landscape is foundational before evaluating genetic therapies for rare diseases specific to your family's situation.
Pro Tip: Learn the terms in vivo and ex vivo early. When speaking with a specialist or reading a trial description, these two words will immediately tell you whether your cells leave the body during treatment or whether the therapy is delivered directly into you. It changes the risk profile, the logistics, and often the eligibility criteria entirely.
Emerging personalized therapies: N-of-1 and latest advances
For patients with ultra-rare diseases, where sometimes only a dozen people worldwide share the same mutation, standard gene therapy development simply doesn't happen. The economics don't support it. This is precisely where N-of-1 therapies are changing everything.

An N-of-1 therapy is designed for a single patient. It starts with a complete genomic analysis of the patient's specific mutation, followed by engineering a treatment, often an ASO, a base editor delivered via LNP, or a custom viral construct, targeted to that exact variant. The timeline from diagnosis to treatment can now be compressed to months rather than decades.
The most striking recent example involves CPS1 deficiency, a rare urea cycle disorder. Researchers used base editing delivered via lipid nanoparticles to correct the patient's specific mutation. The infant's condition stabilized within weeks. This was not a clinical trial in the traditional sense. It was a single patient receiving a fully customized genetic correction, then published to advance the science for others.
Steps in personalized therapy development:
- Full genomic sequencing to identify the exact pathogenic variant
- Functional validation in patient-derived cells (often iPSCs or primary cells)
- Therapeutic design: ASO sequence design, base editing guide RNA, or viral construct
- Safety testing in cellular and animal models
- Regulatory pathway: compassionate use, expanded access, or umbrella trial enrollment
- Manufacturing under GMP (good manufacturing practice) conditions
- Administration at a specialized center with monitoring protocols
| Approach | Patient type | Time to treatment | Outcome example |
|---|---|---|---|
| N-of-1 ASO | Single patient, known splicing variant | 3 to 12 months | Stabilization of neurological decline |
| N-of-1 base editing (LNP) | Infant with metabolic disorder (e.g., CPS1) | 6 to 18 months | Metabolic stabilization within weeks |
| Standard gene therapy (AAV) | Disease with established trial | 1 to 3 years (trial) | Long-term correction (Zolgensma, SMA) |
Pro Tip: Seek care at centers experienced in genomic diagnostics and umbrella trial programs. Programs like URGenT and CHOP's umbrella trial infrastructure are specifically designed to give ultra-rare patients access to cutting-edge personalized options that would otherwise be impossible to reach. Read a detailed evaluation guide for gene therapy to understand how to assess which programs fit your situation. Families who engage these centers early consistently report faster access to personalized rare disease treatments than those who wait for mainstream trial announcements.
FDA-approved gene therapies: Options, outcomes, and patient access
While N-of-1 approaches are exciting, several gene therapies have already cleared the FDA and are available now. Knowing what exists and who qualifies is essential.
Currently approved gene therapies for rare diseases include:
- Zolgensma (onasemnogene abeparvovec): A one-time AAV9-based gene replacement for spinal muscular atrophy (SMA) in children under two. Among the most studied gene therapies in rare disease.
- Waskyra (WAS gene therapy): Approved for Wiskott-Aldrich syndrome (WAS), a rare immunodeficiency.
- Otarmeni: Approved for OTOF-related hearing loss. Critically, Otarmeni is available free in the US under the National Priority Voucher Program, with 80% of patients meeting the primary endpoint in clinical trials.
"Before this approval, families of children with OTOF hearing loss had almost no options. A one-time treatment, available at no cost, that restores meaningful hearing function, is exactly the kind of outcome gene therapy has always promised." — Reflecting the lived experience of families in FDA approval testimonies.
The clinical benchmarks for sickle cell disease (SCD) using exa-cel (Casgevy) are particularly striking: 97% of patients eliminated severe vaso-occlusive crises, with health-related quality of life improvements exceeding the minimum clinically important difference sustained at 36 months. For Canavan disease, a gene therapy trial showed statistically significant reductions in N-acetylaspartate (NAA) levels (P=0.0008) and improved myelination (P=0.0137), both critical biomarkers of disease progression.
Key criteria to access FDA-approved gene therapies:
- Confirmed genetic diagnosis via certified molecular testing
- Age and weight eligibility (particularly strict for Zolgensma)
- Absence of disqualifying anti-AAV antibody titers (for AAV-based products)
- Enrollment or referral through a certified treatment center
- Insurance authorization or enrollment in a patient assistance or Medicaid program
- Completion of pre-treatment workup including liver function, immunology, and cardiac assessments
Understanding the full landscape of FDA-approved rare disease drugs helps families build a realistic picture of what is within reach today. For a deeper look at safety considerations alongside options, explore gene therapy options and safety.
Barriers and practical considerations for families
Even when a therapy exists, getting to it is rarely straightforward. Families consistently run into the same obstacles, and knowing them in advance makes navigation far less painful.
Major challenges include high treatment costs, immune responses, manufacturing scalability, access barriers, and edge cases that exclude patients with pre-existing AAV antibodies or anatomical variations. These are not rare exceptions. They are common enough to derail treatment plans for a significant portion of eligible patients.
"Families often find out their child has high anti-AAV antibody titers only after a referral and months of preparation. Getting that blood test done early, before any referral process begins, is one of the most practical steps any family can take."
How to overcome the top five barriers:
- High cost: Explore outcomes-based Medicaid payment models. The CMS Cell and Gene Therapy Access Model provides outcomes-based agreements specifically designed to expand access for Medicaid-enrolled sickle cell disease patients, a framework likely to expand to other diseases.
- Immune response: Test anti-AAV antibody titers early. Some centers are exploring plasmapheresis or immunosuppression protocols to manage high titers, and knowing your baseline opens doors.
- Manufacturing limits: For N-of-1 therapies, connect with academic medical centers that have GMP manufacturing capabilities on-site. Commercial manufacturers rarely prioritize single-patient runs.
- Anatomical exclusions: Ask your care team to assess anatomical suitability during the initial workup, not after trial enrollment begins. This saves months.
- Lack of advocacy: Patient advocacy organizations can provide navigation support, funding, and direct connections to trial sponsors. Families who engage advocacy early tend to access care faster.
Pro Tip: Early genetic diagnosis and anti-AAV titer screening together are the two single most impactful steps you can take before pursuing any AAV-based gene therapy. Addressing key challenges in rare disease becomes far easier once your baseline data is in hand. Understanding must-know gene therapy approaches will also help you and your care team make faster, better-informed decisions.
Getting started: Practical steps for families seeking gene therapy
Knowing that options exist is one thing. Knowing exactly what to do next is another. Here is a practical checklist for families beginning this process.
Step-by-step checklist:
- Get a full genetic diagnosis. Whole exome or whole genome sequencing through a certified lab is often necessary for ultra-rare cases. Phenotypic diagnosis alone is rarely enough to qualify for trials.
- Request anti-AAV antibody titer testing. This is a simple blood test that can determine eligibility for most AAV-based therapies before you invest significant time in a specific trial.
- Identify specialized centers. Look for programs with active rare disease gene therapy protocols, ideally with on-site genomic diagnostics, GMP manufacturing, and trial coordinators.
- Explore compassionate use and expanded access. The FDA's expanded access program allows patients who don't meet trial criteria to potentially receive investigational treatments if no alternatives exist.
- Enroll in disease registries. Many trials recruit from patient registries. Being registered with the relevant advocacy foundation or academic center dramatically increases your visibility.
- Ask about long-term monitoring. Long-term monitoring is essential due to risks like hepatotoxicity, which may require steroid management. Understanding post-treatment follow-up requirements upfront prevents surprises later.
- Build your care team proactively. The ideal team includes a geneticist, a disease specialist, an immunologist, and a patient navigator or social worker familiar with rare disease systems.
Pro Tip: When you speak with a specialist, ask two specific questions: "What is the expanded access process if my child doesn't qualify for the trial?" and "What does post-treatment monitoring look like for the next five years?" These questions reveal whether the center has the depth of experience your family needs. Consult the gene therapy screening guide to prepare for these conversations with the right clinical vocabulary.
Our perspective: What most families miss about gene therapy for rare diseases
Here is what rarely gets said in the standard patient information materials: gene therapy's greatest promise for ultra-rare diseases is not the blockbuster approvals. It is the N-of-1 model, the idea that a treatment can be designed specifically for your child's exact mutation, tested in cells derived from your child's own body, and administered at a specialized center with the expertise to manage every step. That model is real. It is happening now. And most families have never heard of it.
Researchers behind personalized CRISPR therapies at CHOP are actively designing umbrella trial infrastructure so that individual patients can access custom treatments through a regulatory framework that didn't exist five years ago. This is not future science. This is current clinical practice at select centers.
What families consistently underestimate is the gap between a therapy being approved and a therapy being accessible. Accelerated FDA approvals based on surrogate endpoints move faster than the EMA's more cautious conditional marketing authorization process, but they also create pricing and durability questions that take years to resolve. Outcomes-based payment models are the bridge, but they require active negotiation and advocacy at both the institutional and policy levels.
The families who succeed are not necessarily the ones with the most resources. They are the ones who found the right specialized center early, got the right diagnostic workup done before any trial opened, and stayed engaged with advocacy organizations who could surface opportunities others never saw. Post-treatment monitoring and gene editing explained in plain terms are not afterthoughts. They are the difference between a treatment that holds and one that requires emergency management a year later.
Our advice: do not wait for a cure to be announced. Start building the infrastructure around your family right now.
Explore further: Personalized rare disease solutions and expert support
If this guide has clarified your options, the next step is finding tools and expertise tailored to your specific disease and mutation. Navigating gene therapy alone is genuinely hard, and the difference between knowing what exists and knowing what applies to your family often comes down to having the right support.

RareLabs builds patient-specific disease models from your own cells, runs parallel treatment screens across thousands of FDA-approved compounds and custom ASOs, and evaluates gene therapy options in a rigorous, transparent process designed for families who can't wait. Explore the RareLabs treatment knowledge hub for detailed resources on specific rare diseases, therapy types, and what the science actually supports. When you're ready to take the next step, visit RareLabs to learn how personalized modeling can accelerate the search for your family's answer.
Frequently asked questions
How does gene therapy actually work for rare diseases?
Gene therapy uses delivery systems like AAV or lipid nanoparticles to carry new or modified genetic material into cells, correcting the root defect rather than managing symptoms.
What are N-of-1 gene therapies and who qualifies?
N-of-1 therapies are custom treatments built for a single patient's exact mutation, typically requiring access to specialized genomic diagnostics and centers with clinical trial infrastructure; personalized base editing therapies like the CPS1 case show these can stabilize patients within weeks.
Are FDA-approved gene therapies free or covered by insurance?
Some are: Otarmeni for OTOF hearing loss is available free under the National Priority Voucher Program, while others like Zolgensma may be covered under Medicaid or outcomes-based payment agreements.
What barriers prevent patients from accessing gene therapy?
High costs, immune responses, manufacturing limits, and anatomical exclusions are the most common blockers, but early genetic diagnosis and anti-AAV titer testing can resolve eligibility questions before families invest heavily in a specific pathway.