
Gene editing is not science fiction. Right now, in real clinical settings, physicians are using precise molecular tools to rewrite the DNA responsible for rare and devastating diseases. In fact, one infant received a fully personalized gene editing therapy within roughly six months of diagnosis, marking a turning point for what families facing rare genetic diseases can realistically hope for. This article breaks down how gene editing works, which tools matter most, what the real benefits and risks look like, and how the patient journey from diagnosis to treatment actually unfolds.
Table of Contents
- What is gene editing and how does it work?
- Types of gene editing tools: From CRISPR to precision methods
- Benefits and limitations: What patients and families need to know
- From diagnosis to treatment: The patient-specific gene editing journey
- A closer look: What most guides miss about gene editing for rare diseases
- Find support in your rare disease gene editing journey
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Gene editing defined | Gene editing enables site-specific changes in DNA, opening new possibilities for treating rare genetic diseases. |
| Precision tools evolving | Newer methods like base and prime editing increase accuracy and safety for patient treatments. |
| Real-world results | Personalized gene editing has already helped rare disease patients in clinical settings. |
| Balance of risks and benefits | Not all editing is risk-free, but ongoing assessment helps guide safe decisions for families and patients. |
| Start-to-finish pathway | Gene editing for rare diseases can move from diagnosis to treatment in as little as six months in some cases. |
What is gene editing and how does it work?
Gene editing is a way to make precise, intentional changes to the DNA inside living cells. Unlike older approaches that simply added new genetic material into a cell, gene editing targets a specific location in the genome and modifies, corrects, or removes a sequence that is causing disease. Think of the genome as a very long instruction manual. Gene editing is like having the ability to find a single misprint on one page and fix only that word, without rewriting or replacing the whole document.
The process works by introducing molecular tools into a cell. These tools find the target DNA sequence, make a specific change, and then rely on the cell's own natural repair machinery to finalize the edit. There are two main types of repair: one that cuts and rejoins DNA quickly but somewhat imprecisely (called NHEJ), and one that uses a provided template to make a highly accurate repair (called HDR, or homology-directed repair). The type of repair used depends on the goal and the editing technology chosen.
Genome editing definition (NIST): Gene editing involves site-specific modifications to a DNA sequence, using the cell's natural repair or recombination processes to achieve the desired genetic change.
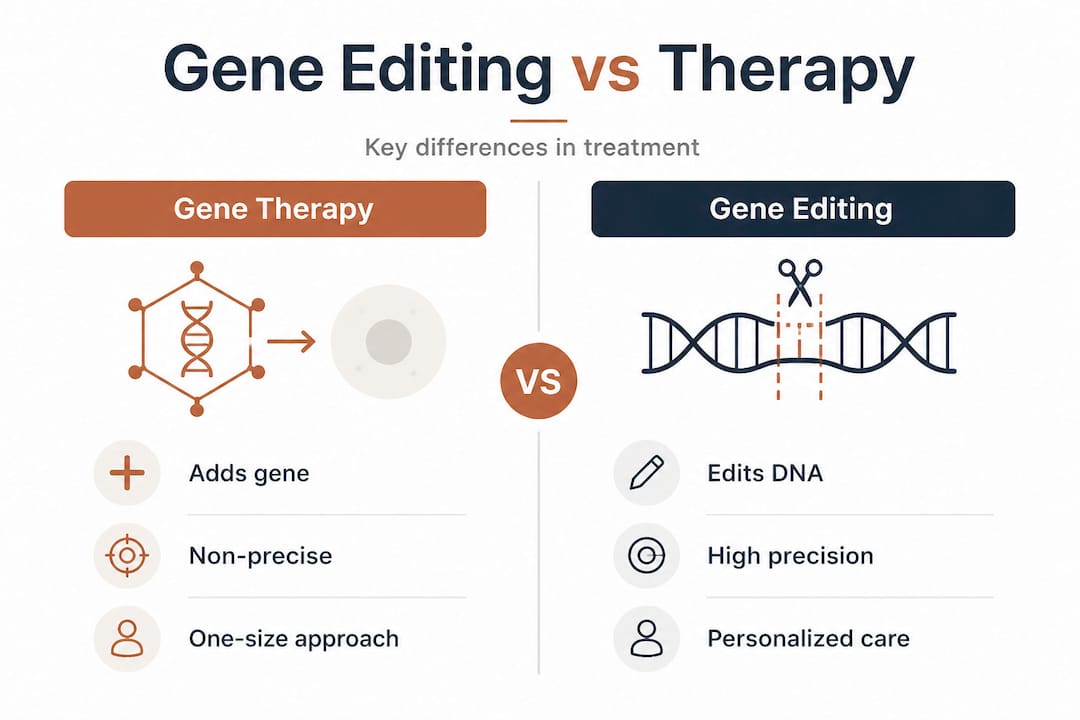
It is important to understand that gene editing differs meaningfully from traditional gene therapy. Traditional gene therapy typically delivers a working copy of a gene into a cell so the cell has something functional to use. Gene editing, on the other hand, actually changes the existing DNA. This distinction is significant because it means gene editing can correct the root cause of a disease, not just work around it. For families exploring genetic therapies for ultra-rare diseases, understanding this difference is the first step toward knowing which approach may apply to your situation.
| Feature | Traditional gene therapy | Gene editing |
|---|---|---|
| What it does | Adds a functional gene copy | Modifies the existing DNA sequence |
| Durability | Varies; may not persist long-term | Often designed for lasting effects |
| Precision | Lower; gene inserts at random locations | High; targets a specific genomic site |
| Personalization potential | Limited | Very high |
Types of gene editing tools: From CRISPR to precision methods
With a foundation in what gene editing does, the next step is understanding which tools are shaping modern therapies. Not all gene editing technologies are the same. Each carries its own mechanism, strengths, and trade-offs, especially when applied to rare diseases where every detail of the mutation matters.
CRISPR (Clustered Regularly Interspaced Short Palindromic Repeats) is the most widely recognized tool. It uses a guide RNA to direct a protein called Cas9 to a specific DNA location, where it makes a precise double-stranded cut. The cell then repairs this cut, and researchers take advantage of this repair to disrupt a gene, remove a harmful sequence, or insert a correction. CRISPR-based systems cut DNA at selected sites and recruit the cell's own repair machinery to introduce the desired change.
Base editing is a newer approach that skips the double-stranded cut entirely. Instead of slicing the DNA, base editors chemically convert one DNA letter into another, for example changing a C to a T. This is valuable because a significant portion of disease-causing mutations are single-letter changes, and base editing can correct these with remarkable accuracy. There is less risk of unintended large deletions because the DNA strand is never fully broken.
Prime editing goes a step further. Often described as a "search and replace" function for the genome, prime editing can correct all 12 possible point mutations, small insertions, and small deletions. It uses a modified guide RNA carrying the corrected sequence directly. Base editing and prime editing expand therapeutic options precisely because they avoid double-stranded breaks, reducing the chances of unintended genomic rearrangements.
For a deeper look at how these fit into a broader strategy, the overview of gene therapy approaches for ultra-rare diseases provides helpful context.
Key advantages of modern gene editing in rare disease treatment:
- Ability to correct a mutation at its exact source, not just compensate for it
- Potential for a single treatment to provide long-lasting benefit
- Growing capacity to design patient-specific therapies for unique mutations
- Newer tools like base and prime editing reduce risk of unintended DNA damage
- Can be applied to cells inside the body (in vivo) or to cells taken out, edited, and returned (ex vivo)
Pro Tip: When your loved one's mutation is a single-letter change in the DNA, precision tools like base editing or prime editing may offer a safer and more targeted option than standard CRISPR cuts. Always ask the research team which editing tool is being considered and why.
| Tool | Mechanism | Precision | Typical use in rare diseases |
|---|---|---|---|
| CRISPR/Cas9 | Double-stranded DNA cut | Moderate to high | Gene disruption, large corrections |
| Base editing | Single-base chemical conversion | Very high | Single-point mutation correction |
| Prime editing | Search and replace with template | Highest | Point mutations, small insertions/deletions |
Benefits and limitations: What patients and families need to know
Understanding how these tools are used in practice brings us to the concrete benefits they promise, alongside the realistic limitations every patient and family must weigh carefully before moving forward.
The most significant benefit of gene editing is durability. When a correction is made to the DNA inside a patient's own cells, that correction can persist for the lifetime of those cells. For somatic cells (meaning cells in the body that are not passed to future generations), a successful edit can mean a lasting, nonheritable fix. Gene editing in rare diseases aims for this kind of permanent, somatic correction for individual patients, which is a fundamentally different promise from therapies that need to be repeated indefinitely.
Another key advantage is personalization. Because the mutation causing a rare disease is often unique to one patient or one small group of patients, gene editing tools can be designed specifically around that mutation. A custom guide RNA, a tailored base editor, or a prime editing construct can be built for a patient who has no existing commercial treatment available.
The limitations are real and important. Off-target effects (unintended edits at locations in the genome other than the target) remain one of the primary concerns in gene editing. Off-target effects and genomic consequences are inherent risks, and perfect accuracy is not achievable with any current technology. Not every rare disease is suitable for gene editing, either. Some conditions involve multiple genes, large deletions, or are caused by mechanisms that editing tools cannot yet address efficiently.
On managing expectations: Off-target effects must be evaluated not just for their presence, but for whether they occur in critical regions of the genome and what risk they realistically carry. Context and expert assessment are everything.
Benefits of gene editing for rare diseases:
- Long-lasting effect from a single intervention
- Targets the root genetic cause
- High personalization potential for ultra-rare mutations
- Growing delivery options including lipid nanoparticles (tiny fat particles that carry the editing tools into cells)
Limitations and risks to discuss with your care team:
- Off-target edits, even when rare, require careful monitoring
- Not all tissues or cell types are easily accessible for editing
- Long-term safety data is still accumulating
- Delivery of the editing tool to the correct cells in the body remains a technical challenge
- Regulatory approval timelines can be lengthy for personalized therapies
For a full overview of what to realistically expect, the guide on gene therapy risks and expectations and information on personalized treatment pathways offer family-focused context.
Pro Tip: When evaluating safety, ask researchers specifically where in the genome any off-target edits were detected and whether those locations are associated with cancer risk or other functional consequences. Not all off-target activity carries the same level of concern.
From diagnosis to treatment: The patient-specific gene editing journey
Now, let's walk through exactly what the journey looks like when gene editing is applied to create a personalized therapy, from the first diagnosis through to receiving treatment.
The story of a child diagnosed with CPS1 deficiency, an ultra-rare metabolic disorder affecting the liver, illustrates this journey clearly. CPS1 deficiency causes toxic ammonia to build up in the blood, which can cause severe neurological damage or death. There was no approved treatment, no existing gene therapy. Yet within roughly six months of diagnosis, in vivo gene editing of liver cells was designed and delivered specifically for this patient. The child showed measurable improvement.
From the NIH report: "The infant became the first person to receive a fully customized in vivo base editing therapy, with the treatment designed and tested within months of the diagnosis."
This case is not typical yet, but it shows what is becoming possible. Here is the general pathway:
- Genetic diagnosis confirmed. Whole genome or exome sequencing identifies the precise mutation causing the disease.
- Mutation analysis. Scientists assess whether the specific mutation is correctable with existing gene editing tools.
- Therapy design. A guide RNA and editing tool (CRISPR, base editor, or prime editor) are custom-built for the patient's exact mutation.
- Preclinical testing. The therapy is tested in cell models or animal models to confirm it works and identify any safety signals, including off-target effects.
- Regulatory review. For personalized therapies under emergency compassionate use, regulators can sometimes expedite review.
- Delivery and treatment. The editing tool is delivered into the patient's body, often via lipid nanoparticles or viral vectors (modified viruses used as delivery vehicles), and administered under clinical supervision.
- Monitoring and follow-up. Ongoing assessment tracks both the therapeutic benefit and any unintended genomic changes.
The gene therapy evaluation guide can help you understand what questions to ask at each step. And if you are just beginning to explore options, the guide to finding rare disease treatments lays out a practical starting framework.
The timeline from diagnosis to treatment in the clinical case above was approximately six months. While many situations will take longer due to the complexity of the disease, the regulatory environment, or access to expert labs, this case sets a benchmark for what rapid, patient-specific science can achieve.
A closer look: What most guides miss about gene editing for rare diseases
Most articles about gene editing focus almost exclusively on the technology itself. They explain CRISPR mechanics, list tools, and describe clinical trials. What they miss is the decision framework that matters most to patients and families actually facing a diagnosis.
Here is what we observe: families often come to us after reading everything they can find, and they are still asking the wrong questions. They ask, "Is this the best technology?" when they should be asking, "Is this the right approach for my specific mutation, in my specific tissue, at this point in my child's disease progression?"
Precision does not just mean editing precisely. It means asking precisely the right questions. The difference between somatic editing (changing cells in a living patient's body with no effect on future children) and germline editing (changing eggs, sperm, or early embryos, which would be heritable) is one of the most critical distinctions in all of medicine. Nearly all therapeutic gene editing today is somatic. Germline editing remains ethically restricted and scientifically premature. Families should not be confused or misled by coverage that blurs these two very different things.
The evaluation framework matters as much as the science itself. When exploring ex vivo gene therapy options, for example, the key questions are not just about efficacy. They are about which cells will be edited, how they will be returned to the body, and what monitoring will be in place afterward.
Essential questions every family should ask:
- Is this therapy targeting somatic cells only, with no heritable changes?
- What specific editing tool is being used and why was it chosen over alternatives?
- How were off-target effects assessed, and in what cell type?
- What follow-up monitoring is planned and for how long?
- Is there an independent safety monitoring board reviewing this protocol?
- What happens if the therapy does not achieve the intended effect?
The families who navigate this process most effectively are not those who know the most about CRISPR. They are the ones who ask structured, specific questions and demand transparent answers. Build your evaluation checklist early, before you are in a room being asked to sign a consent form under emotional pressure.
Find support in your rare disease gene editing journey
Navigating gene editing options for a rare disease is one of the most complex and emotional experiences a family can face. You should not have to do it alone or without expert guidance.

At RareLabs, we specialize in helping patients and families explore exactly these options, from understanding which editing tools may apply to a specific mutation, to identifying research programs and evaluating potential pathways. Our team builds personalized disease models from patients' own cells and runs rigorous treatment screens, including gene therapy evaluation. Whether you are at the earliest stage of a diagnosis or already weighing specific clinical options, the RareLabs Knowledge search is a practical starting point for exploring the most current gene editing research and resources available for your disease. We are built for the cases that conventional medicine has not yet solved.
Frequently asked questions
Is gene editing a permanent cure for rare genetic diseases?
Gene editing in somatic cells aims for lasting effects, but whether it constitutes a complete cure depends heavily on the disease type, the tissue targeted, and the editing tool used. Gene editing can be designed for durable in vivo effects, though long-term data is still accumulating for most conditions.
What is the difference between gene editing and gene therapy?
Gene editing makes precise changes to the existing DNA sequence, while traditional gene therapy delivers a working gene copy without altering the patient's original sequence. Gene editing enables targeted changes that address the root mutation directly, which is a key distinction in how therapies are designed and what outcomes are possible.
How long does it take to go from diagnosis to personalized gene editing treatment?
Timelines vary significantly, but recent clinical reports show it is possible in some cases within roughly six months. The process from diagnosis to completed in vivo gene editing treatment was approximately six months in one landmark case, though most situations will take longer depending on disease complexity and regulatory pathways.
What are off-target effects in gene editing and should I worry about them?
Off-target effects are unintended edits that occur elsewhere in the genome, and while modern tools minimize them significantly, zero risk does not exist. Off-target risk is inherent and requires practical evaluation by experts who can assess which off-target changes matter clinically and which do not.