The workflow for undiagnosed disease patients is a coordinated process in which patients compile their full medical history, engage multidisciplinary specialist teams, and pursue structured evaluation through specialized programs to reach a diagnosis. The standard industry term for this process is the "clinical diagnostic pathway," though patients and families often encounter it described simply as the undiagnosed disease workflow. The average time to diagnosis for a rare disease ranges from 4 to 7 years. That delay is not inevitable. A structured approach cuts through the fragmentation that causes most of those lost years.
What does the workflow for undiagnosed disease patients require to start?
Every effective diagnostic pathway begins with one document: a unified, chronological medical record. This file should include every symptom, test result, imaging report, specialist note, and hospitalization, organized by date. Without this foundation, even the best multidisciplinary team cannot connect the dots across organ systems.
Patients have a legal right to request this information. Under HIPAA and the 21st Century Cures Act, you are entitled to your complete records, not just the summary your patient portal displays. Request full lab results, imaging files, pathology reports, and physician notes from every provider you have seen.

Several tools support record organization. Patient portals like MyChart aggregate records from participating health systems. AI-assisted platforms such as Unsolved Diagnosis help patients synthesize complex histories into formats clinicians can quickly review. Programs like the Undiagnosed Diseases Network (UDN) require consent forms and eligibility screening before submission, so having your records organized in advance prevents delays at that stage.
Key items to gather before submitting to any program:
- Chronological symptom timeline with dates, severity, and triggers
- All genetic testing reports, including raw data files when available
- Imaging studies on disc or in digital format, not just written summaries
- Specialist notes from every physician who has evaluated you
- A list of all medications tried and their outcomes
Pro Tip: Request records directly from each hospital's medical records department, not only through your patient portal. Portals often omit imaging files, pathology slides, and older notes that predate the digital system.
What does the step-by-step evaluation process involve?
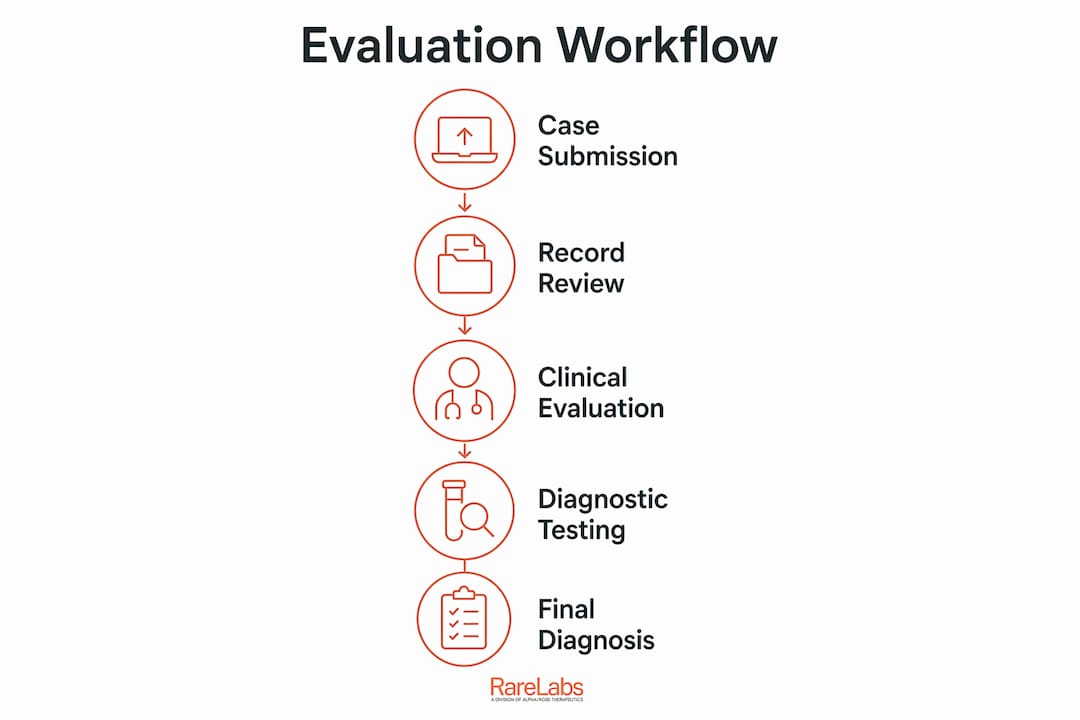
The evaluation process follows a defined sequence. Understanding each stage prevents confusion and helps you prepare the right materials at the right time.
- Case submission. You submit your organized records, consent forms, and a written symptom summary to a program such as the UDN or a hospital-based undiagnosed conditions clinic.
- Eligibility review. A nurse coordinator or intake team screens your case for completeness and program fit. Incomplete files are returned, which adds weeks to the timeline.
- Medical record synthesis. A nurse coordinator compiles records from multiple health systems into a single clinical summary. This step is more complex than a standard second opinion because it requires cross-system data integration.
- Multidisciplinary team review. Specialists from neurology, genetics, immunology, and other relevant fields review the case together. Academic medical centers and specialized programs look across organ systems for patterns that individual specialists miss.
- Evaluation and testing. The team may order targeted new tests, recommend imaging, or request additional genetic panels based on their review.
- Outcome communication. Patients receive one of three outcomes: a diagnosis, a recommendation for further testing, or a determination that no current program resource can assist.
The UDN's medical record review can take up to 60 business days after all records are received. That timeline reflects the depth of review, not a backlog. Patient navigators are available through the UDN at no charge to guide families through each stage.
A standard second opinion differs significantly from a comprehensive undiagnosed conditions program. Programs like the Cedars-Sinai Virtual Second Opinion involve multiple specialists reviewing your case simultaneously, rather than one physician offering a single perspective. That parallel review structure is what makes these programs effective for complex, multi-system presentations.
Pro Tip: Ask your patient navigator to confirm receipt of every document you submit. Missing a single imaging file can restart the 60-day review clock.
| Stage | Who is involved | Typical timeline |
|---|---|---|
| Case submission | Patient, family | 1–2 weeks to prepare |
| Eligibility review | Nurse coordinator | 1–2 weeks |
| Record synthesis | Nurse coordinator | 2–4 weeks |
| Multidisciplinary review | Specialist team | Up to 60 business days |
| Outcome communication | Care team, navigator | Varies by case |
How can patients and families actively accelerate the diagnosis process?
Patients who take an active role in their own case move faster through the clinical workflow for undiagnosed patients. The single most impactful thing you can do is maintain a structured symptom timeline. Clinicians connect disparate observations far more quickly when they can see a clear chronological record of what happened, when, and in what order.
Genetic testing results deserve special attention. Negative results should be reanalyzed periodically because new gene-phenotype associations emerge as medical knowledge grows. A test that returned no findings in 2020 may yield a diagnosis when reanalyzed against a 2026 gene database. Ask your geneticist to schedule a formal reanalysis every one to two years.
Common pitfalls that slow the process:
- Submitting portal summaries instead of complete records
- Assuming a "normal" genetic test means genetics is ruled out
- Waiting for one specialist to refer you to the next, rather than proactively contacting programs directly
- Failing to update your symptom timeline after new developments
- Not informing your care team when symptoms change or worsen
Collecting complete records from multiple providers is harder than most patients expect. Hospitals use different electronic health record systems, and records from providers seen years ago may require written requests and processing fees. Start this process early, before you submit to any program.
Pro Tip: Keep a living document, updated monthly, that logs every new symptom, medication change, and specialist visit. Share this document with every new clinician you see. It saves hours of intake time and reduces the risk of critical details being overlooked.
What specialized programs and resources exist for undiagnosed patients?
Several programs exist specifically for patients who have not received a diagnosis after standard medical evaluation. They vary in focus, access requirements, and what they offer.
| Program | Focus | Access |
|---|---|---|
| Undiagnosed Diseases Network (UDN) | Rare and undiagnosed genetic conditions | Application-based, U.S. patients |
| Cedars-Sinai Virtual Second Opinion | Multi-system undiagnosed conditions | Fee-based, available nationally |
| NIH Undiagnosed Diseases Program | Research-driven evaluation | Referral and application required |
| Academic medical center clinics | Broad multidisciplinary review | Referral often required |
The UDN is the most structured entry point for patients in the United States. It connects patients to a network of academic medical centers, each with dedicated multidisciplinary teams. The program is research-funded, which means evaluation is provided at no cost to accepted patients.
Academic medical centers outside the UDN also offer value. Their multidisciplinary teams bring a fresh perspective to cases that have stalled in community hospital settings. The key difference is that these teams review all systems simultaneously rather than sequentially.
Technology is changing what is possible in identifying undiagnosed conditions. AI-assisted workflows synthesize multimodal clinical data, including genomics, imaging, and lab trends, to propose diagnostic hypotheses that fragmented care misses. A 2026 study in NEJM AI highlighted the growing role of large language model-assisted workflows in rare disease diagnosis. Platforms like Unsolved Diagnosis apply this approach directly to patient cases. Research into peptide array screening also shows promise for identifying biomarkers in cases where standard panels return no findings.
Patient support organizations such as the National Organization for Rare Disorders (NORD) and Global Genes provide educational resources, peer support networks, and guidance on insurance navigation. Insurance coverage for specialized programs varies widely. Contact your insurer before enrolling in any fee-based program to confirm what is covered.
Key Takeaways
The most effective workflow for undiagnosed disease patients combines complete, organized medical records with multidisciplinary program evaluation and periodic reanalysis of prior test results.
| Point | Details |
|---|---|
| Start with complete records | Request full files under HIPAA, not just patient portal summaries, before submitting to any program. |
| Use structured programs | The UDN and academic medical centers offer multidisciplinary review that individual specialists cannot replicate. |
| Reanalyze genetic results | Negative genetic tests should be reviewed periodically as new gene-disease associations are discovered. |
| Maintain a symptom timeline | A chronological log of symptoms and encounters is the single most useful document you can give a clinical team. |
| Leverage AI tools | AI-assisted platforms synthesize complex histories and propose hypotheses that traditional fragmented care misses. |
What I've learned after years of watching families navigate this process
The families who move fastest through the undiagnosed disease process are not the ones with the most severe cases. They are the ones who treat their medical records like a legal case file. Every document is organized, dated, and cross-referenced. Every new symptom is logged the day it appears. That discipline is not natural for most people dealing with a sick child or a frightening personal diagnosis. But it is the single variable that most consistently separates families who get answers from those who wait years longer.
The second thing I have observed is that most patients underestimate how different a true multidisciplinary review is from a series of individual specialist appointments. Seeing a neurologist, then a rheumatologist, then a geneticist in sequence is not the same as having all three review your case together. The cross-specialty conversation is where diagnoses are made. Programs like the UDN exist precisely because that conversation rarely happens in standard care. If you have been through multiple specialists without answers, the problem is almost certainly the structure of the evaluation, not the complexity of your case.
I also want to be honest about the emotional weight of this process. Waiting 60 business days for a record review while your child is symptomatic is genuinely hard. The workflow does not eliminate that difficulty. What it does is give you something concrete to do at every stage, which is far better than waiting passively. You can read more about communicating findings with your care team to make every appointment count.
— John
How Hopeatrarelabs supports patients seeking rare disease answers
Hopeatrarelabs works with patients and families who are still searching for answers after standard diagnostic pathways have stalled. Their approach goes beyond diagnosis support by building patient-specific disease models from the patient's own cells, then testing thousands of FDA-approved drugs and custom therapies against those models.

For patients who have a suspected or confirmed rare disease and need to understand what treatment options exist, the Hopeatrarelabs Knowledge base is a searchable resource covering rare disease research and therapy information. It is designed to complement the diagnostic workflow by giving patients and families access to current treatment data and research updates. You can also visit Hopeatrarelabs directly to learn how their personalized treatment search process works and whether your case qualifies for evaluation.
FAQ
How long does the undiagnosed disease workflow typically take?
The diagnosis process for rare diseases averages 4 to 7 years from symptom onset. Structured programs like the UDN can compress the evaluation phase, but record preparation and eligibility review add weeks before clinical review begins.
What records do I need before submitting to a program like the UDN?
You need complete records, including lab results, imaging files, pathology reports, specialist notes, and genetic testing data. Partial summaries from patient portals are not sufficient for program evaluation.
Can a negative genetic test be revisited later?
Yes. Periodic reanalysis of genetic results is recommended because new gene-disease associations are discovered regularly. A negative result from several years ago may yield a diagnosis when reviewed against current databases.
What is the difference between a second opinion and an undiagnosed disease program?
A standard second opinion involves one physician reviewing your case. An undiagnosed disease program, such as those at Cedars-Sinai or the UDN, involves multiple specialists from different fields reviewing your case simultaneously, which is what makes them effective for multi-system presentations.
Where can families find support during the diagnostic process?
Organizations like NORD and Global Genes offer peer support, educational resources, and insurance guidance. Patient navigators through the UDN are available at no cost and can guide families through every stage of the clinical evaluation process.