
Parallel treatment screening is defined as the simultaneous testing of many potential therapies against a patient's disease model to maximize the chance of finding one that works. For families facing rare or undiagnosed genetic diseases, this approach is not optional. It is the method most likely to find an answer before disease progression closes the window. Sequential testing, which evaluates one therapy at a time, risks exhausting both time and precious biological samples before a match is found. Parallel screening solves both problems at once, and the science behind why it works is worth understanding in full.
Why parallel treatment screening is the right approach for rare diseases
Parallel treatment screening follows what diagnosticians call the OR rule: a patient's disease model is declared responsive if any tested therapy produces a positive result. This maximizes sensitivity by ensuring no potentially effective treatment is missed. The trade-off is a higher rate of false positives, meaning some flagged therapies will require follow-up validation before clinical use. That trade-off is entirely acceptable when the alternative is missing the one drug that could help.
Serial testing, by contrast, follows the AND rule. Each test must confirm the last before the next begins. This approach maximizes specificity, reducing false positives but dramatically increasing the risk of false negatives. In a rare disease context, a false negative means a potentially life-saving therapy goes undetected. That cost is far too high.

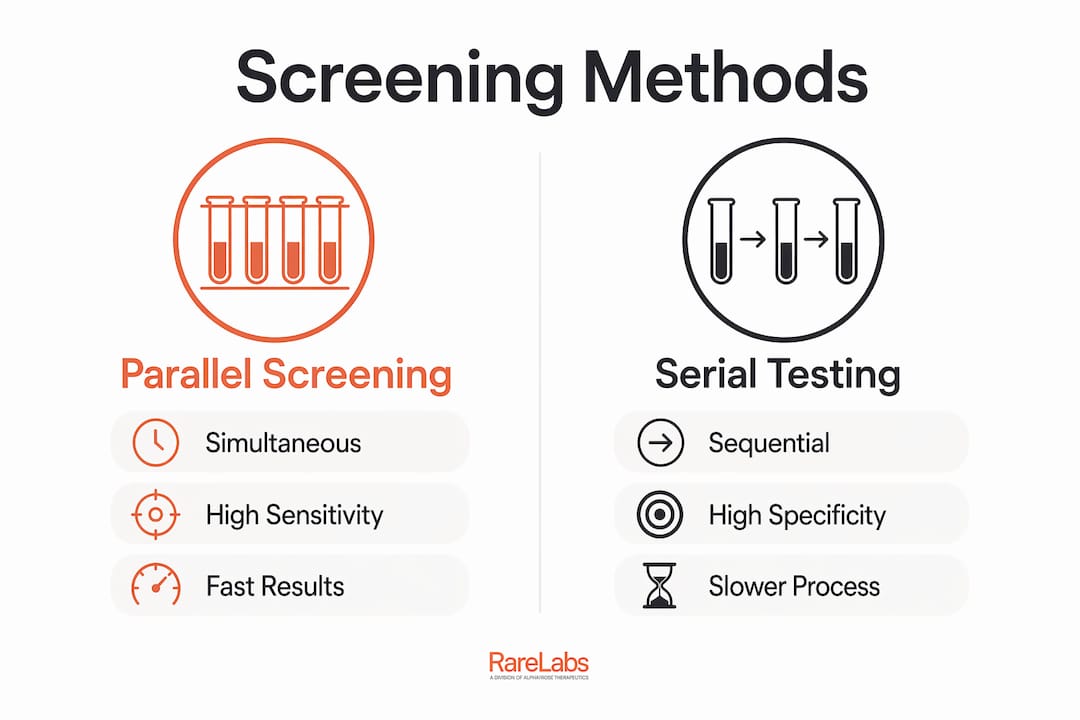
The table below shows how these two approaches differ across the criteria that matter most to patients and families.
| Criteria | Parallel screening | Serial testing |
|---|---|---|
| Testing order | Simultaneous | Sequential |
| Primary goal | Maximize sensitivity | Maximize specificity |
| False negative risk | Low | High |
| Sample use | Efficient, tested once | High, tested repeatedly |
| Speed to result | Faster | Slower |
| Best suited for | Ultra-rare, urgent cases | Low-prevalence, confirmatory |
Pro Tip: Ask your care team whether the screening approach being used follows a parallel or serial design. If your disease is ultra-rare, parallel is the clinically justified choice.
Why rare and undiagnosed diseases demand concurrent screening
The cost of a missed therapy in ultra-rare disease is not just medical. It is measured in months of disease progression, lost function, and in some cases, life. This is why the clinical decision framework for rare diseases consistently favors parallel approaches over serial ones.
Three factors make concurrent screening especially critical in this population:
- Sample scarcity. Patient-derived cells, whether from a biopsy or an induced pluripotent stem cell (iPSC) model, exist in limited quantities. Serial testing risks exhausting these samples before a match is found. Parallel screening tests many candidates at once, preserving what cannot be replaced.
- Disease urgency. Many rare genetic diseases are progressive. Every week without an effective therapy can mean permanent damage. Parallel screening compresses the discovery timeline.
- No approved treatment baseline. Most ultra-rare diseases have no FDA-approved therapy. Patients cannot fall back on a standard of care. The screening process itself is the primary path to treatment.
When the cost of missing a therapy exceeds the cost of investigating a false positive, parallel screening is not just preferred. It is the only defensible clinical choice. Diagnostic experts confirm that false negative costs in ultra-rare disease screening make parallel testing the superior method, even when it generates more leads requiring follow-up.
Hopeatrarelabs applies this logic directly. The lab tests thousands of FDA-approved drugs, custom antisense oligonucleotides (ASOs), and gene therapy candidates simultaneously against patient-specific iPSC disease models. The goal is to leave no viable option untested.
Pro Tip: If your family is navigating an undiagnosed genetic disease, ask specifically whether the lab uses iPSC-derived models. These patient-specific models allow parallel screening without requiring repeated invasive sample collection.
For a practical overview of how to begin this process, the step-by-step treatment guide from Hopeatrarelabs walks families through each stage.
How modern technology makes parallel screening faster and more accurate
The practical challenge of testing thousands of drug candidates simultaneously is significant. Automated AI-assisted workflows have changed what is possible. A human-in-the-loop screening pipeline tested across 27 clinical trials demonstrated 94% criterion-level agreement at approximately $0.12 per patient. That level of accuracy at that cost was not achievable with manual review alone.
The key is the hybrid model. AI handles the high-volume pattern recognition across large compound libraries. Human scientists then validate flagged results, catching errors that automation alone would miss. This combination improves both speed and safety in a way that neither approach achieves independently.
Data standardization is equally important. Protocols like HL7 FHIR allow clinical data from multiple sources to be centralized and made compatible. A unified screening framework using HL7 FHIR reduced data abstraction time by up to 80% in oncology settings. That same efficiency gain applies directly to rare disease treatment screening, where pulling together fragmented patient records is often the biggest bottleneck.
Practical factors that determine whether a parallel screening program succeeds include:
- Centralized data access. All relevant patient records, genomic data, and prior test results must be accessible before screening begins.
- Standardized data formats. Inconsistent data formats slow analysis and introduce errors. HL7 FHIR compliance is the current benchmark.
- Human validation checkpoints. Automated results require expert review before any clinical decision is made.
- Pre-planned workflows. Retrofitting parallel screening into a rigid existing process creates integration failures. Workflow design must happen before the first sample is processed.
For families interested in how gene therapy candidates fit into this process, the gene therapy screening guide from Hopeatrarelabs explains the specific steps involved.
What patients and families should expect during the screening process
Parallel treatment screening follows a defined sequence, even though many tests run at the same time. Understanding each step helps families ask the right questions and set realistic expectations.
- Sample collection. A small biological sample, often blood or a skin biopsy, is collected. This sample is used to create a patient-specific iPSC disease model that replicates the patient's genetic condition in a lab dish.
- Disease model creation. Scientists use CRISPR gene editing and iPSC technology to build a model that behaves like the patient's affected cells. This model becomes the testing platform for all drug candidates.
- Parallel drug screening. Thousands of compounds are applied to the disease model simultaneously. FDA-approved drugs, ASOs, and gene therapy options are all evaluated in the same round.
- Automated analysis. AI systems analyze the results across all tested compounds, flagging those that show a meaningful response.
- Human expert validation. Scientists review every flagged result. Promising candidates are confirmed through secondary assays before any recommendation is made.
- Results and next steps. Families receive a report detailing which therapies showed activity and what the recommended next steps are, including whether any candidates are available for compassionate use or clinical trial enrollment.
Pro Tip: Before screening begins, ask the lab how results will be communicated and what the timeline looks like. Knowing when to expect updates reduces anxiety and helps families plan.
The rare disease answers guide from Hopeatrarelabs provides additional context on accelerating this process in 2026.
Limitations and challenges families should understand
Parallel screening is the best available method for rare disease therapy discovery. It is not perfect. Understanding its limitations helps families engage with the process realistically.
The most common challenge is false positives. Because parallel screening prioritizes sensitivity, some flagged therapies will not hold up under secondary validation. This is expected and manageable, but it means the initial results list is a starting point, not a final answer. Follow-up testing is always required before any clinical use.
Other challenges include:
- Data quality gaps. If a patient's medical records are incomplete or stored in incompatible formats, the screening process slows down. Families can help by gathering and organizing records before the process begins.
- Sample limitations. Even with iPSC modeling, some patients have conditions that make reliable model creation difficult. Labs with deep experience in rare disease modeling, like Hopeatrarelabs, have protocols to address this, but it remains a real constraint.
- Workflow integration. Clinicians and researchers who attempt to add parallel screening to an existing serial workflow without redesigning the process often encounter delays and errors. Proper planning before implementation is not optional.
- Interpretation complexity. Results from a parallel screen require expert interpretation. Families should expect to work with a specialist who can translate lab findings into clinical decisions.
Emerging improvements in AI and data interoperability are steadily reducing these barriers. The challenges in rare disease research continue to shrink as standardization improves and more patient data becomes available for analysis.
Key Takeaways
Parallel treatment screening is the most effective method for rare disease therapy discovery because it maximizes sensitivity, preserves limited samples, and uses AI-assisted workflows with human validation to find answers faster.
| Point | Details |
|---|---|
| Parallel beats serial for rare diseases | Simultaneous testing finds more viable therapies and avoids missing the one drug that could help. |
| Sample preservation matters | iPSC-based parallel screening tests thousands of candidates without exhausting irreplaceable patient cells. |
| AI plus human oversight is the standard | Hybrid pipelines achieve over 94% accuracy while keeping expert scientists in the validation loop. |
| Data standardization drives speed | HL7 FHIR-compatible frameworks cut data abstraction time by up to 80%, accelerating results. |
| False positives require follow-up | Initial parallel screen results are a starting point; expert validation confirms which candidates are clinically relevant. |
What I've learned watching parallel screening change rare disease outcomes
The families I've seen benefit most from parallel treatment screening share one thing: they asked for it early. Not after a year of serial testing had exhausted their samples and their options. Early, when the disease model was fresh and the compound library was fully available.
The shift toward AI-assisted workflows has been real and meaningful. But the families who get the most out of it are the ones who treat the process as a collaboration, not a black box. They ask questions. They push for human expert review of every flagged result. They share their data with research networks so that the next family facing the same mutation has a faster path.
What I find underappreciated is the role of data quality in determining outcomes. A lab can run the most sophisticated parallel screen in the world, but if the patient's records arrive fragmented and incompatible, the process stalls. Families who invest time in organizing their medical history before screening begins consistently see faster, cleaner results.
The other thing worth saying plainly: parallel screening does not always find an answer. But it finds answers far more often than serial testing does, and it does so without burning through the biological material that cannot be replaced. For a family with a child facing a disease that has no approved treatment, that difference is everything.
— John
How Hopeatrarelabs supports your parallel screening process
Hopeatrarelabs was built specifically for patients and families who cannot afford to wait for a sequential process to run its course.

The lab creates patient-specific iPSC disease models from your own cells, then runs a full parallel screen across thousands of FDA-approved drugs, custom ASOs, and gene therapy candidates simultaneously. Every result goes through expert human validation before it reaches you. The RareLabs Knowledge platform gives families direct access to treatment search tools, trial matching, and the research findings generated through this process. If you are looking for a place to start, that platform is where the most current information lives.
FAQ
What is parallel treatment screening?
Parallel treatment screening tests many potential therapies against a patient's disease model at the same time, following an OR rule to maximize the chance of finding an effective treatment. It is the preferred method for rare diseases where missing a viable therapy carries a high cost.
How does parallel screening differ from serial testing?
Serial testing evaluates one therapy at a time and requires each test to confirm the last before proceeding. Parallel screening runs all candidates simultaneously, which is faster, preserves more sample material, and reduces the risk of missing an effective therapy.
Why is sensitivity more important than specificity in rare disease screening?
In ultra-rare diseases, the cost of a false negative, missing a therapy that could have helped, far exceeds the cost of a false positive that requires follow-up testing. Diagnostic decision frameworks consistently favor sensitivity in these high-stakes scenarios.
What role does AI play in parallel treatment screening?
AI-assisted pipelines analyze large compound libraries rapidly and flag candidates showing meaningful activity. Human scientists then validate every flagged result, a hybrid approach that achieves over 94% accuracy while maintaining clinical safety standards.
Can parallel screening work if my family member has limited biological samples?
Yes. Labs like Hopeatrarelabs use iPSC technology to create a renewable disease model from a small initial sample. This means thousands of drug candidates can be tested without requiring repeated invasive collection or risking sample exhaustion.