
CRISPR technology is defined as a gene-editing system derived from the natural immune defense of bacteria, enabling scientists to locate, cut, and modify specific DNA sequences with a level of precision that older methods could not match. The system uses two core components: a guide RNA that targets a specific genetic address, and the Cas9 enzyme that acts as molecular scissors to cut the DNA at that location. The NIH and FDA have both recognized CRISPR's clinical potential, with the FDA approving the first CRISPR-based therapy, exagamglogene autotemcel, for clinical use. Phase 3 trials for hereditary angioedema also succeeded as of april 2026, marking a turning point for in vivo gene editing. For researchers and patients navigating rare genetic diseases, CRISPR gene editing represents one of the most consequential tools in modern medicine.
What is CRISPR technology and where does it come from?
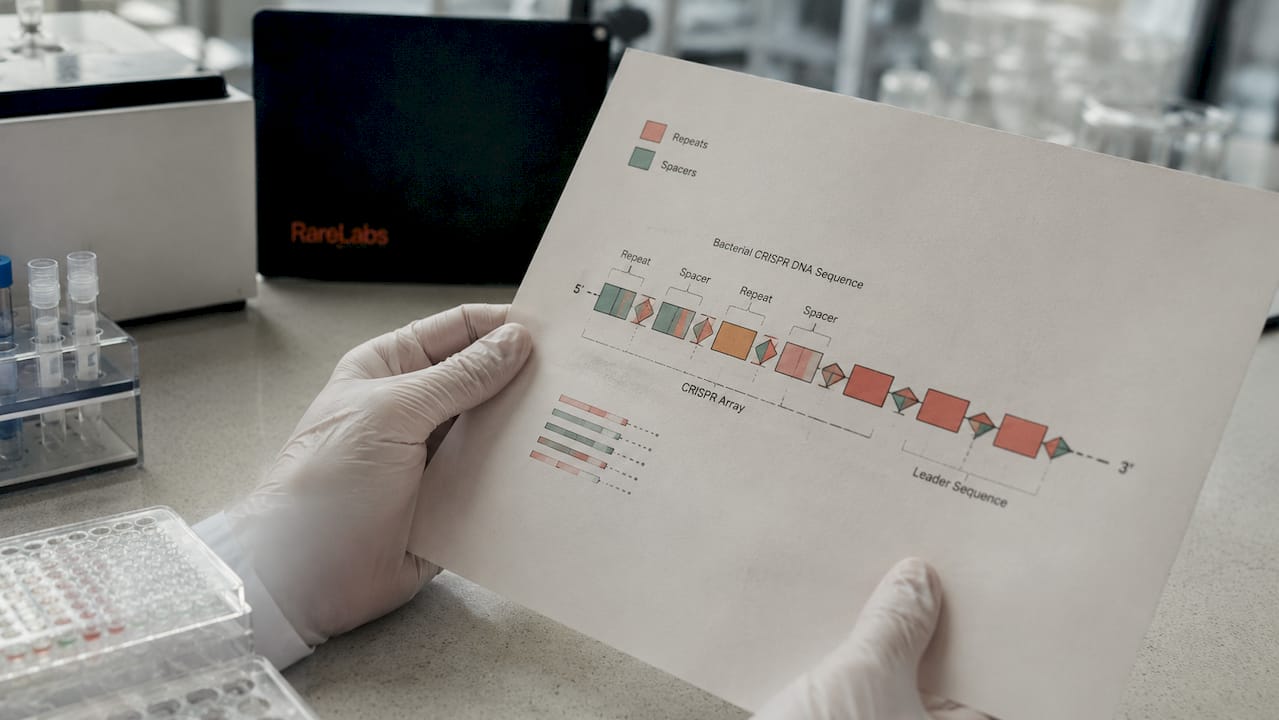
CRISPR stands for Clustered Regularly Interspaced Short Palindromic Repeats. The name describes a pattern scientists first noticed in bacterial DNA: short, repeated sequences separated by unique spacers. Those spacers are not random. They are fragments of viral DNA that bacteria captured during past infections, stored as genetic memory.
CRISPR sequences exist in approximately 50% of bacterial genomes and 90% of archaea. That prevalence tells you this is not a niche adaptation. It is one of the most widespread immune strategies in microbial life. When a virus attacks again, the bacterium transcribes those stored sequences into guide RNAs, which direct Cas proteins to the matching viral DNA and cut it apart.
Scientists recognized that this targeting system could be reprogrammed. Instead of pointing at viral DNA, a custom guide RNA could direct Cas9 to any sequence in any genome. That insight transformed a bacterial defense mechanism into a universal gene-editing platform. The biological logic is elegant: the same system that protects bacteria from viruses now gives researchers the ability to rewrite the human genome.
Key features of the natural CRISPR system include:
- Genetic memory storage: Bacteria insert viral DNA fragments between CRISPR repeats after surviving an infection.
- Guide RNA production: When the same virus returns, the bacterium produces RNA copies of those stored fragments.
- Cas protein activation: Guide RNAs recruit Cas proteins, which scan incoming DNA for a matching sequence.
- Targeted cleavage: Once a match is found, the Cas protein cuts the viral DNA, neutralizing the threat.
- Heritable immunity: Offspring inherit the CRISPR array, passing the immune memory to the next generation.
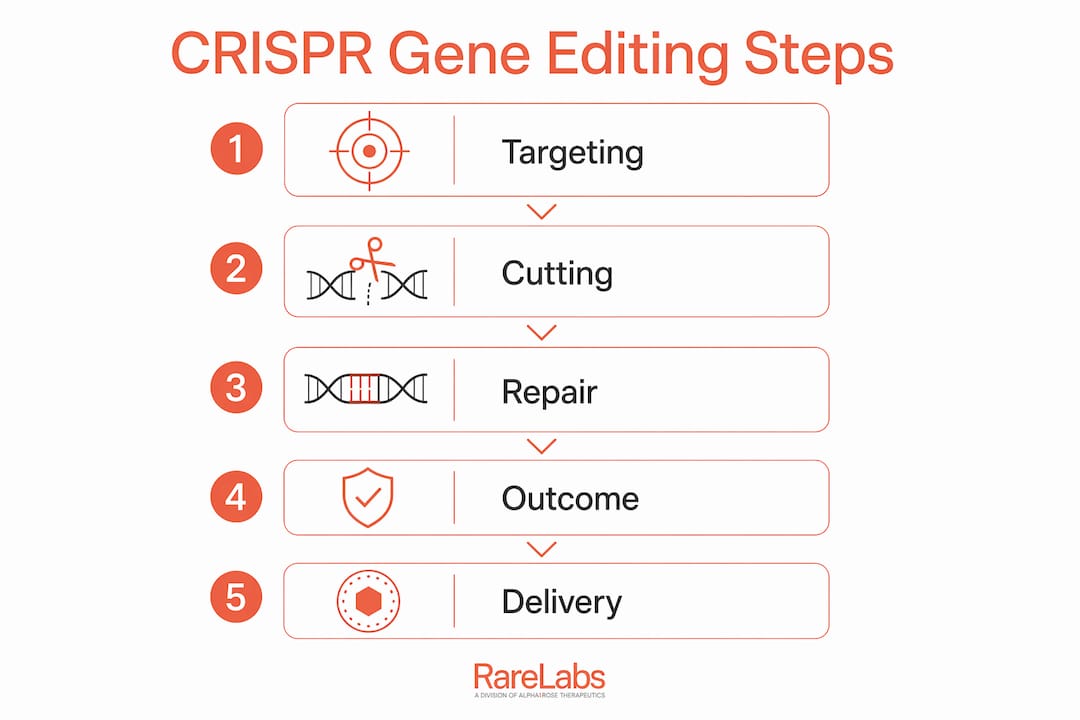
How does CRISPR-Cas9 enable precise gene editing?
CRISPR-Cas9 works through a two-part targeting system. A synthetic guide RNA is designed to match the DNA sequence a researcher wants to edit. The Cas9 enzyme binds to that guide RNA and travels along the genome until it finds a complementary sequence. It then makes a double-strand break, cutting both strands of the DNA helix.
What happens next depends on the repair pathway the cell uses. The cell can rejoin the cut ends imprecisely, which typically disables the gene. Alternatively, if a DNA template is provided alongside the CRISPR components, the cell uses that template to repair the break, inserting or substituting specific sequences. This gives researchers three core editing outcomes: deletion, insertion, or substitution.
Older gene-editing tools like zinc finger nucleases (ZFNs) and TALENs also cut DNA, but they required custom protein engineering for every new target. Designing a new ZFN took months. Designing a new CRISPR guide RNA takes days. That difference in speed and cost is why CRISPR displaced those methods so quickly across research labs worldwide.
Delivery method matters as much as the edit itself. The two main strategies are:
- Ex vivo editing: Cells are removed from the patient, edited in a lab setting, and reinfused. This approach allows thorough quality control before any edited cells re-enter the body.
- In vivo editing: CRISPR components are packaged into delivery vehicles, such as lipid nanoparticles, and administered directly to the patient. The in vivo approach targets organs like the liver through intravenous infusion.
- High-fidelity Cas9 variants: Engineered versions of Cas9 reduce the chance of cutting at unintended genomic sites, improving safety for clinical applications.
- Off-target validation: Before any clinical use, extensive genomic sequencing is required to confirm that edits occurred only at the intended location.
Pro Tip: When evaluating a CRISPR-based therapy in a clinical trial, ask specifically whether the delivery method is ex vivo or in vivo. The answer determines the risk profile, the manufacturing complexity, and the monitoring requirements for the patient.
For a deeper look at how these delivery strategies apply to rare diseases, the ex vivo gene therapy overview from Hopeatrarelabs breaks down the practical differences clearly.
What are the current clinical and research applications of CRISPR?
CRISPR's clinical track record is no longer theoretical. The FDA-approved therapy exagamglogene autotemcel treats sickle cell disease by editing patients' own stem cells to produce functional hemoglobin. Separately, a Phase 3 trial for hereditary angioedema succeeded as of april 2026, demonstrating that in vivo CRISPR editing of liver genes produces durable effects with no waning over six months. These results confirm that CRISPR has crossed from laboratory promise into clinical reality.
Beyond blood disorders, CRISPR applications span several fields:
- Monogenic diseases: Single-gene disorders like sickle cell disease and beta-thalassemia are the most tractable targets because one edit addresses the root cause.
- Cancer immunotherapy: Researchers edit T cells to improve their ability to recognize and destroy tumor cells, a strategy now in multiple clinical trials.
- Agriculture: CRISPR in crops enables site-specific gene knockouts and insertions to improve yield, disease resistance, and nutritional profiles with greater efficiency than older breeding methods.
- Epigenome editing: Using catalytically inactive Cas9 (dCas9), researchers can modulate gene activity without cutting DNA at all, opening safer treatment options for complex disorders.
| Application area | Example | Current stage |
|---|---|---|
| Sickle cell disease | Exagamglogene autotemcel | FDA approved |
| Hereditary angioedema | In vivo liver editing | Phase 3 success (2026) |
| Cancer immunotherapy | Edited T cell therapies | Multiple Phase 1/2 trials |
| Crop improvement | Yield and resistance edits | Commercial development |
| Epigenome modulation | dCas9-based gene regulation | Preclinical to early clinical |
The breadth of these applications explains why researchers describe CRISPR as transformative rather than incremental. No prior gene-editing platform reached this many disease areas this quickly. For researchers working on genetic therapies for ultra-rare diseases, CRISPR's flexibility makes it a central tool in the treatment development pipeline.
What challenges and ethical considerations surround CRISPR?
Off-target editing is the most immediate technical challenge. CRISPR can cut at genomic sites that resemble the intended target, potentially disrupting genes unrelated to the disease being treated. High-fidelity Cas9 variants reduce this risk, but they do not eliminate it. Every clinical program requires rigorous sequencing-based validation before a therapy reaches patients.
In vivo delivery adds another layer of complexity. Lipid nanoparticles and viral vectors must reach the right tissue, avoid triggering an immune response, and release CRISPR components at effective concentrations. The delivery challenges for in vivo editing are substantially harder than for ex vivo approaches, where quality control happens outside the body.
The language clinicians use around CRISPR outcomes reflects genuine scientific caution. Gene-editing experts describe CRISPR therapies as "functional cures" or "durable disease modifications" rather than permanent cures. Long-term monitoring is required to verify that edits remain stable over a patient's lifetime. That distinction matters for patients making treatment decisions.
Ethical regulation remains crucial as gene-editing precision improves. The clinical focus stays on serious diseases, but the same tools that treat sickle cell disease could theoretically be applied to non-therapeutic traits. Community advocacy, transparent regulatory oversight from bodies like the FDA, and public education are all necessary to manage those societal implications responsibly.
Pro Tip: If you are reviewing a CRISPR clinical trial for a rare disease patient, check whether the trial protocol includes long-term genomic monitoring at defined intervals. Trials that lack this component have a weaker safety evidence base.
What is the future outlook for CRISPR gene editing?
The next wave of CRISPR development moves away from DNA cutting entirely. Defanged CRISPR platforms using catalytically inactive Cas9 (dCas9) modulate gene expression without creating double-strand breaks. This approach reduces the risk of permanent unintended alterations, making it a more viable strategy for common complex disorders where permanent edits carry greater risk.
New CRISPR-like systems are also entering the field. The Fanzor system, discovered in eukaryotic organisms, represents a naturally occurring RNA-guided nuclease outside the bacterial CRISPR family. Its smaller size may make it easier to package into delivery vehicles, potentially solving one of the persistent constraints of in vivo delivery.
Phase 3 clinical pipelines are expanding. Multiple programs targeting liver diseases, blood disorders, and inherited blindness are in late-stage trials. Regulatory agencies including the FDA are developing clearer frameworks for reviewing gene-editing therapies, which should accelerate approval timelines for well-characterized programs.
The long-term implication for regenerative medicine is significant. CRISPR-based tools could eventually correct disease-causing mutations in patient-derived induced pluripotent stem cells (iPSCs), generate personalized disease models, and screen therapies before any treatment reaches the patient. Hopeatrarelabs already applies iPSC technology alongside CRISPR gene editing to build patient-specific models for ultra-rare diseases, translating this future vision into current practice.
Key Takeaways
CRISPR gene editing is the most consequential advance in molecular medicine in decades, with FDA-approved therapies, Phase 3 successes, and a growing pipeline that spans blood disorders, liver diseases, and cancer immunotherapy.
| Point | Details |
|---|---|
| Biological origin | CRISPR is a natural bacterial immune system reprogrammed for precise human gene editing. |
| Core mechanism | Guide RNA directs Cas9 to a target DNA sequence, where it cuts and enables deletion, insertion, or substitution. |
| Clinical milestone | The FDA approved exagamglogene autotemcel; Phase 3 hereditary angioedema trials succeeded in 2026. |
| Delivery distinction | Ex vivo editing allows pre-infusion quality control; in vivo delivery targets organs directly but requires sophisticated vectors. |
| Future direction | Defanged dCas9 platforms modulate gene expression without DNA cuts, reducing permanent alteration risks. |
Why CRISPR's pace still surprises me
I have followed gene-editing research for years, and the speed of CRISPR's translation from bacterial curiosity to approved therapy still catches me off guard. Most molecular tools spend decades in preclinical work before reaching a single patient. CRISPR moved from published mechanism to FDA-approved therapy in roughly a decade.
What I find underappreciated is the distinction between ex vivo and in vivo delivery. Most public coverage treats CRISPR as a single technology, but those two delivery strategies have almost nothing in common from a clinical risk standpoint. Ex vivo editing is closer to a manufacturing process. In vivo editing is closer to a drug. Conflating them leads to unrealistic expectations in both directions.
The ethical debate also tends to focus on germline editing, which remains prohibited in clinical practice. The more immediate concern is access. CRISPR therapies for sickle cell disease currently cost over a million dollars per patient. The science is advancing faster than the reimbursement frameworks. That gap will define who actually benefits from this technology over the next decade.
The researchers and clinicians I respect most in this field are the ones who insist on calling these therapies "functional cures" rather than permanent fixes. That precision is not pessimism. It is the honest acknowledgment that we are still learning how edited genomes behave over a lifetime. The science is extraordinary. The humility to keep monitoring it is what makes it safe.
— John
Hopeatrarelabs and the search for rare disease treatments
Rare diseases present a specific challenge that general CRISPR coverage rarely addresses: most patients with ultra-rare or undiagnosed genetic conditions have no approved therapy at all. Hopeatrarelabs addresses that gap directly.

The RareLabs Knowledge hub compiles the latest research on gene-editing approaches, FDA-approved therapies, and emerging clinical trials relevant to rare genetic diseases. Hopeatrarelabs builds patient-specific disease models using iPSCs and CRISPR gene editing, then screens thousands of FDA-approved drugs and custom antisense oligonucleotides (ASOs) against those models. For patients, families, and physicians who need more than a literature search, the rare disease treatment search platform provides a structured, scientifically rigorous starting point.
FAQ
What is CRISPR technology in simple terms?
CRISPR is a gene-editing system that uses a guide RNA and the Cas9 enzyme to find and cut specific DNA sequences. Scientists can then disable, repair, or replace genes at that location.
What diseases can CRISPR treat?
CRISPR currently has an FDA-approved therapy for sickle cell disease and has shown Phase 3 success for hereditary angioedema. Active research programs target cancer, inherited blindness, and liver diseases.
What is the difference between ex vivo and in vivo CRISPR editing?
Ex vivo editing removes cells from the patient, edits them in a lab, and reinfuses them. In vivo editing delivers CRISPR components directly into the body, typically targeting organs like the liver through lipid nanoparticles.
Are CRISPR therapies permanent cures?
Clinical experts describe CRISPR outcomes as "functional cures" or "durable disease modifications" rather than permanent cures. Long-term genomic monitoring is required to confirm that edits remain stable over a patient's lifetime.
What are the main risks of CRISPR gene editing?
The primary risks are off-target edits at unintended genomic sites and immune responses triggered by delivery vehicles. High-fidelity Cas9 variants and rigorous sequencing validation reduce these risks before any therapy reaches patients.