Cellular models are defined as laboratory-grown human cell systems used to test how drugs behave in living tissue before clinical trials begin. The role of cellular models in drug discovery has become foundational, particularly for rare and undiagnosed genetic diseases where animal models routinely fail to replicate human pathology. New approach methodologies (NAMs), the recognized industry term for this class of tools, now span 2D monolayer cultures, 3D organoids, and organ-on-chip platforms. The FDA Modernization Act 3.0 formally recognizes NAMs as complementary or replacement testing platforms, signaling a regulatory shift that researchers can no longer afford to ignore. For diseases affecting fewer than 200,000 patients in the United States, these models are often the only path to a testable hypothesis.
What is the role of cellular models in drug discovery?
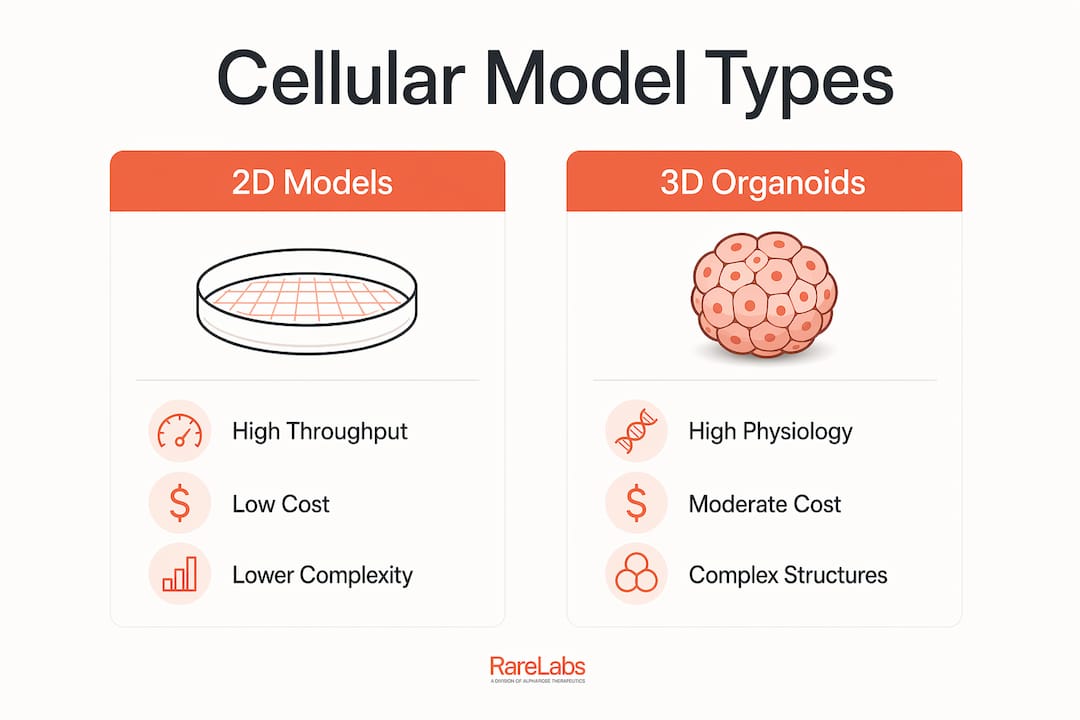
Cellular models give researchers a human-relevant system to screen compounds, measure toxicity, and study disease mechanisms. Traditional 2D monolayer cultures, where cells grow flat on a plastic surface, remain the workhorse of early-stage in vitro drug testing because they are fast, inexpensive, and easy to scale. Their limitation is equally well known: cells in a flat layer lose the three-dimensional architecture that governs how they actually respond to drugs.
3D organoids address that gap directly. These self-organizing cell clusters replicate organ-specific structures, including the spatial relationships between cell types that control gene expression and drug metabolism. Human-centric NAMs include primary cells, immortalized lines, and stem-cell-derived 3D structures, all of which show increasing regulatory acceptance. That acceptance matters because it means data generated from these platforms can now support regulatory submissions.

Organoids-on-chip, also called microphysiological systems, add fluid flow and mechanical forces to 3D cultures. They replicate the dynamic environment of living tissue more closely than any static model. For rare disease research, where patient samples are scarce, the ability to extract maximum information from minimal material is not a convenience. It is a scientific necessity.
| Model type | Physiological relevance | Throughput | Cost | Best use case |
|---|---|---|---|---|
| 2D monolayer | Low | High | Low | Initial compound screening |
| 3D organoid | High | Medium | Medium | Disease modeling, toxicity |
| Organoids-on-chip | Very high | Low | High | Drug metabolism, safety |
| Patient-derived iPSC | Very high | Medium | High | Precision medicine, rare disease |
Pro Tip: When selecting a model type, match complexity to the question. Use 2D assays for high-throughput compound triage, then validate hits in 3D or patient-derived systems before committing resources to animal studies.
How do cellular models improve drug efficacy and safety prediction?
Animal models predict human drug responses poorly in many disease categories. Species-specific differences in receptor pharmacology, metabolic enzymes, and immune signaling mean that a compound safe in rodents can be toxic in humans, and vice versa. This translational gap is a primary driver of late-stage clinical trial failures.
Liver organoids-on-chip demonstrate high sensitivity in detecting hepatotoxicity and can categorize toxicity levels that conventional 2D models and animal studies miss entirely. These platforms simulate sinusoidal liver structures with endothelial and hepatocyte interaction, replicating drug metabolism kinetics that closely match clinical data. That level of fidelity allows researchers to identify safe dose ranges far earlier in the development pipeline.
The practical benefits of advanced cellular assays in drug development include:
- Earlier toxicity detection: 3D liver models flag hepatotoxic compounds before costly animal studies begin.
- Species-independent data: Human cell-based systems eliminate the guesswork of cross-species extrapolation.
- Dose-response precision: Organoids-on-chip generate pharmacokinetic data that maps directly to clinical parameters.
- Reduced attrition: Catching failures earlier cuts the financial and time cost of late-stage program termination.
Integrating cellular models with AI and computational tools creates a predictive infrastructure that systematically improves clinical trial success probabilities. The combination is not additive. It is multiplicative: AI identifies patterns across large cellular assay datasets that no human analyst could process manually, then feeds those patterns back into model design.
Pro Tip: Pair your organoid toxicity data with pharmacogenomic testing, such as PGx profiling, to contextualize drug response variation across patient genetic backgrounds before scaling any compound.
What is the role of patient-derived cellular models in rare disease drug discovery?
Patient-derived cellular models are the most direct application of the importance of cell models in precision medicine. They are generated from a patient's own cells, reprogrammed into induced pluripotent stem cells (iPSCs) using Yamanaka factors, and then differentiated into the disease-relevant cell type. The result is a living replica of the patient's genetic disease in a dish.
Patient-derived organoids enable individualized drug response profiling, especially for rare genetic, neurological, and oncological diseases. CRISPR gene editing integrates directly into this workflow, allowing researchers to introduce or correct specific mutations and observe downstream effects on drug sensitivity. For undiagnosed diseases, where the causal variant may be unique to a single patient, this approach is the only way to generate mechanistic data.
The numbered benefits and pitfalls of patient-derived models are worth stating plainly:
- Genetic fidelity: The model carries the patient's exact mutation, including modifier variants that animal models cannot replicate.
- Drug repurposing potential: Screening FDA-approved compounds against patient-specific cells identifies candidates without starting from scratch.
- Functional genomics: CRISPR perturbation screens reveal which genes drive disease phenotype and which are druggable.
- Therapy validation: Gene therapy vectors and antisense oligonucleotides (ASOs) can be tested for efficacy before any clinical exposure.
- Batch variability risk: Genetic and epigenetic differences between iPSC lines from the same patient can produce inconsistent drug response data. Cross-validation with multiple lines is not optional.
- Differentiation efficiency: Not all cell types differentiate with equal efficiency, and immature cells may not express the disease phenotype fully.
Hopeatrarelabs builds patient-specific disease models using iPSC technology and CRISPR editing, then runs parallel treatment screens across thousands of FDA-approved drugs, custom ASOs, and gene therapy options. That workflow directly addresses the precision medicine gap that genetic disease modeling exposes for ultra-rare conditions.
Pro Tip: Always generate at least three independent iPSC clones per patient before drawing conclusions about drug response. Single-clone data is a hypothesis, not a finding.
What are the current technical and regulatory challenges for cellular models?
The main adoption barrier for cellular models is not purely biological. It involves technical and regulatory complexities that require coordinated effort across biology, engineering, and policy to resolve. Researchers entering this space encounter several concrete obstacles:
- Maturation paradox: Achieving full organ-like metabolic function in 3D organoids requires complex microfluidic perfusion and long-term culture, which reduces throughput and increases cost.
- Missing systemic components: Organoids-on-chip lack integrated immune systems and vascular networks, limiting their ability to model systemic drug clearance and immune-mediated adverse effects.
- Reproducibility: Batch-to-batch variability driven by genetic and epigenetic differences remains a critical pitfall, particularly for patient-derived lines.
- Regulatory integration: Despite FDA Modernization Act 3.0, standardized validation frameworks for NAMs in regulatory submissions are still maturing.
- Cost and scalability: Organoids-on-chip platforms remain expensive and technically demanding, restricting access to well-resourced institutions.
"Cellular models are not simply replacements for animal models. They represent a paradigm shift offering ethically sound and physiologically relevant systems essential for overcoming translational gaps in drug research. Realizing that potential requires coordinated advances in bioengineering, standardization, and regulatory science."
Emerging solutions include vascularized organoid systems, immune-competent co-cultures, and AI-driven optimization of culture conditions. Regulatory reforms under FDA Modernization Act 3.0 are actively enabling this shift, incorporating cellular approaches as both complementary and replacement testing platforms. The regulatory direction is clear. The execution timeline is not.
How are cellular models shaping the future of rare disease drug discovery?
The field is moving toward fully human-centric drug development pipelines, and cellular models are the structural foundation of that shift. Several trends are converging to accelerate this transition:
- NAMs replacing animal studies: Human-centric new approach methodologies are supplanting animal models where human drug response prediction is the priority, driven by both higher failure rates in traditional approaches and ethical pressure.
- AI integration: Combining cellular model data with AI-driven computational predictions creates a rapidly iterating predictive infrastructure that shortens development timelines.
- Multi-organoid co-cultures: Advances in vascularization, immune competence, and multi-organoid systems are addressing the systemic integration gap that single-organ platforms cannot resolve.
- Drug repurposing at scale: Patient-derived models enable high-throughput screening of FDA-approved drugs against disease-specific cell lines, identifying viable candidates without the cost of de novo development.
- Digital pathology integration: Pairing cellular model outputs with digital pathology analysis adds a morphological layer to functional drug response data, improving phenotypic characterization.
For rare disease researchers, the practical implication is direct. The combination of patient-derived iPSCs, CRISPR functional genomics, and AI-assisted compound screening now makes it possible to generate a testable therapeutic hypothesis for a single patient within months, not years.
Pro Tip: Track the FDA's evolving NAMs guidance documents alongside your experimental design. Aligning your cellular assay protocols with emerging regulatory standards now reduces the friction of translating preclinical findings into an IND application later.
Key Takeaways
Patient-derived cellular models, combined with AI and regulatory reforms under FDA Modernization Act 3.0, now form the most direct path to therapeutic discovery for rare and undiagnosed genetic diseases.
| Point | Details |
|---|---|
| Model selection matters | Match model complexity to the research question: 2D for screening, 3D or iPSC for disease modeling. |
| Hepatotoxicity detection | Liver organoids-on-chip detect drug-induced liver injury with higher sensitivity than 2D models or animal studies. |
| Patient-derived models enable precision medicine | iPSC-based models carry the patient's exact genetic background, enabling individualized drug response profiling. |
| Batch variability is a real risk | Validate findings across at least three independent iPSC clones before drawing conclusions about drug response. |
| Regulatory alignment accelerates translation | Designing cellular assays to meet FDA Modernization Act 3.0 standards reduces friction when moving toward clinical application. |
Why cellular models changed how I think about rare disease research
The most persistent misconception I encounter is that cellular models are simply better animal models. They are not. They represent a fundamentally different epistemology for drug discovery. Animal models ask: "Does this compound work in a surrogate organism?" Cellular models ask: "Does this compound work in human tissue carrying this specific disease mechanism?" That is not a refinement. It is a different question entirely.
What I have observed in practice is that the researchers who get the most out of these platforms are the ones who treat model selection as a scientific decision, not a technical default. Choosing a 3D organoid because it sounds more sophisticated than a 2D assay is a mistake. Choosing it because the disease phenotype requires three-dimensional cell architecture is sound reasoning.
The rare disease context sharpens this further. When you are working with a patient who has no approved treatment and possibly no published literature on their specific variant, the cellular model is not a screening tool. It is the primary evidence base. That responsibility demands rigor in clone selection, differentiation validation, and cross-validation that many labs underestimate until they are already committed to a compound.
My recommendation for researchers entering this space: invest in your validation framework before you invest in your screening library. A well-characterized patient-derived model with documented batch consistency will generate more credible data from 50 compounds than a poorly characterized model will from 5,000.
— John
Hopeatrarelabs and cellular model-based rare disease research
Hopeatrarelabs builds patient-specific disease models for ultra-rare and undiagnosed genetic diseases, using iPSC technology and CRISPR gene editing to create the cellular systems that make precision drug screening possible.

The RareLabs Knowledge platform gives researchers, physicians, and biopharma partners access to research resources that support personalized cellular model data integration and treatment search strategies. If you are working on a rare disease program and need a rigorous, patient-centric cellular modeling approach, Hopeatrarelabs provides the scientific infrastructure to move from genetic diagnosis to testable therapeutic candidates with speed and transparency.
FAQ
What are cellular models in drug discovery?
Cellular models are laboratory-grown human cell systems, including 2D cultures, 3D organoids, and organ-on-chip platforms, used to test drug efficacy and safety before clinical trials. They are the core of new approach methodologies (NAMs) recognized under FDA Modernization Act 3.0.
How do patient-derived organoids help rare disease research?
Patient-derived organoids carry the patient's exact genetic mutations, enabling individualized drug response profiling and CRISPR-based functional genomics for diseases with no existing treatment options.
What is the maturation paradox in 3D organoids?
The maturation paradox refers to the challenge that achieving full organ-like metabolic function in 3D organoids requires complex microfluidic perfusion systems, which increases cost and reduces throughput compared to simpler 2D assays.
Why do organoids-on-chip still have limitations?
Organoids-on-chip currently lack integrated immune systems and vascular networks, which limits their ability to model systemic drug clearance and immune-mediated adverse effects across multiple organs.
How does FDA Modernization Act 3.0 affect cellular model use?
FDA Modernization Act 3.0 formally recognizes human-centric NAMs, including cellular models, as complementary or replacement testing platforms, enabling their data to support regulatory submissions and reducing reliance on animal studies.