
Orphan drug designation is one of the most misunderstood regulatory concepts in rare disease medicine. Many patients and advocates assume it means a treatment has been approved and is ready to use. It does not. What is orphan drug designation, exactly? It is a formal regulatory status granted to drugs targeting diseases that affect very small patient populations, designed to make development financially viable when it otherwise would not be. Understanding the distinction between designation and approval, and knowing how the system actually works, matters enormously if you are navigating rare disease treatment options for yourself or someone you care about.
Table of Contents
- Key takeaways
- What is orphan drug designation and who qualifies
- Orphan drug benefits that make development possible
- How to apply for orphan designation
- FDA vs. EMA: key differences at a glance
- Impact on treatment availability for rare disease patients
- My perspective on what orphan designation really means
- How Hopeatrarelabs supports your rare disease research
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Designation is not approval | Orphan drug status signals regulatory intent and grants incentives, not permission to market a drug. |
| Two major programs exist | The FDA and EMA run separate orphan designation programs with different thresholds, timelines, and benefits. |
| Financial incentives are significant | Sponsors receive tax credits, fee waivers, and years of market exclusivity to offset development risk. |
| Apply early in development | Submitting an orphan drug application before marketing approval maximizes available incentives and funding opportunities. |
| Gaps remain despite progress | Only about 10% of rare diseases have approved treatments, so designation alone does not guarantee a therapy reaches patients. |
What is orphan drug designation and who qualifies
The orphan drug definition comes down to a simple premise: some diseases affect so few people that no pharmaceutical company would develop a treatment on market economics alone. Without financial incentives, those patients go without options. Orphan drug designation is the regulatory mechanism created to fix that gap.
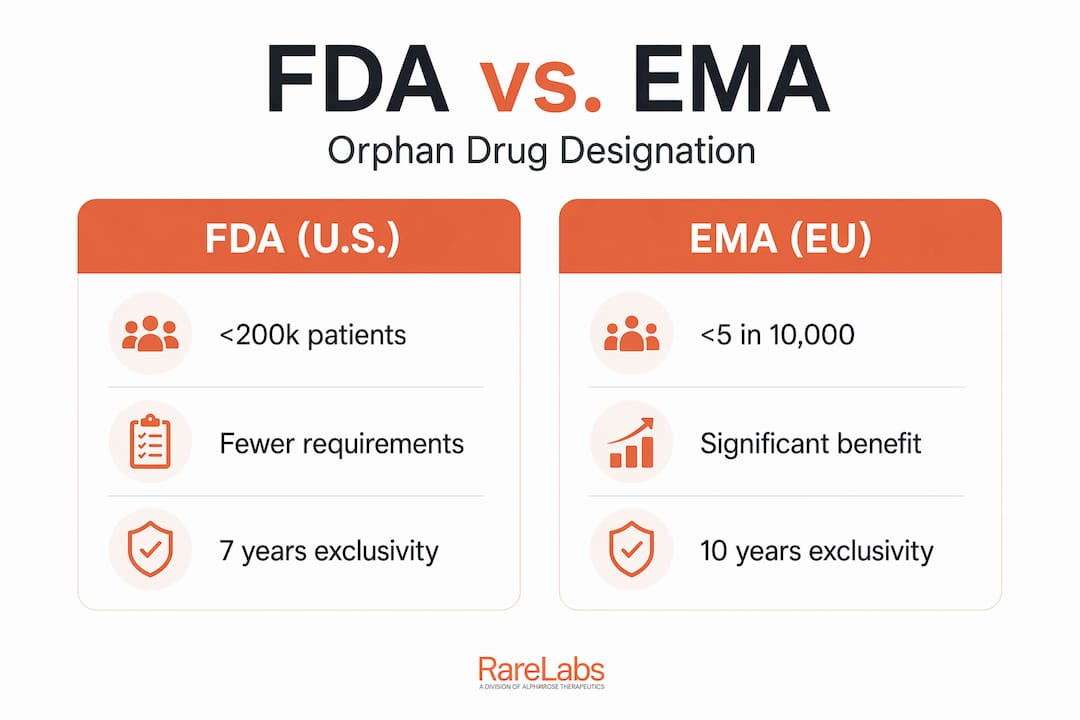
In the United States, the Orphan Drug Act of 1983 established the threshold that still applies today. A disease must affect fewer than 200,000 people in the U.S., or a sponsor must demonstrate that developing the drug would not recover costs through U.S. sales alone. The FDA's Office of Orphan Products Development (OOPD) evaluates these requests. One important point that trips up many researchers: FDA eligibility is based on U.S. prevalence only. A disease affecting millions globally but fewer than 200,000 Americans still qualifies.
The European Medicines Agency (EMA) uses a different measure. In the EU, orphan designation applies when a condition affects no more than 5 in 10,000 people, or when it is life-threatening and inadequately treated. The EMA also requires evidence that the drug offers significant benefit over existing methods. These are meaningful differences that affect strategy for global drug developers.
The criteria for orphan drug status, broken down:
- U.S. (FDA): Fewer than 200,000 affected in the U.S., or no reasonable expectation of cost recovery from U.S. sales
- EU (EMA): Prevalence of no more than 5 in 10,000, or a life-threatening/chronically debilitating condition with no satisfactory existing treatment
- Both require: Evidence of scientific plausibility that the drug addresses the condition, along with prevalence data from published sources or patient registries
- Neither program grants designation based on global population size or commercial market projections outside their respective territories
The orphan drug definition is purely regulatory, not medical. A drug can carry orphan designation and still fail in clinical trials. Designation opens doors; it does not guarantee anything beyond those doors.
Orphan drug benefits that make development possible
The entire logic of orphan drug designation rests on incentives. Without them, the math of rare disease drug development simply does not work. Here is what sponsors gain from FDA orphan designation:
- 7 years of market exclusivity after approval, meaning the FDA will not approve a competing drug for the same indication during that window
- Tax credits up to 25% of qualified clinical trial costs, a meaningful offset for trials that may enroll only dozens of patients
- Waiver of Prescription Drug User Fees, which can exceed $4 million per application
- Enhanced access to FDA guidance through protocol assistance during development
In the EU, the EMA offers 10 years of market exclusivity, extendable by 2 years for sponsors that comply with a pediatric investigation plan. Fee reductions and free protocol assistance from the EMA's Committee for Orphan Medicinal Products make early scientific alignment far more accessible, particularly for smaller biotech firms.
One nuance that sponsors miss: exclusivity is not automatic upon designation. It attaches only after marketing approval, and it can be revoked if the sponsor cannot demonstrate clinical superiority over a previously approved treatment or fails to supply adequate quantities to meet patient demand. Designation gives you the right to earn exclusivity. It does not guarantee it.
Pro Tip: If you are a sponsor evaluating whether to pursue orphan designation, calculate the fee waiver value alongside tax credit projections before the IND stage. For many early-stage rare disease programs, those two incentives alone can offset a significant portion of Phase 1 costs.
The financial risk reduction enabled by these incentives is exactly why drugs like Gleevec and synthetic EPO, originally developed for narrow rare disease indications, eventually reached patients and transformed treatment models across broader conditions.
How to apply for orphan designation
The orphan drug application process is more accessible than most sponsors expect, but precision matters. Here is how it works in practice:
- Determine eligibility first. Gather prevalence data from published epidemiological studies, patient registries, or claims databases. The FDA OOPD recommends brief, focused submissions with clear evidence of disease prevalence and plausible treatment rationale. Long, unfocused applications slow the process.
- Apply at the right time. FDA orphan designation applicants may submit at any development stage before marketing approval, and no Investigational New Drug (IND) application is required. For maximum benefit, applying early once animal model efficacy is shown captures all available incentives and strengthens fundraising conversations with investors.
- Prepare your scientific rationale. You need evidence that the drug could plausibly treat the condition, not proof that it works. Preclinical data, mechanistic reasoning, and a clear description of the disease and unmet need are the core components.
- Submit through the correct channel. FDA applications go through the OOPD portal. EMA applications use the IRIS platform with assigned Research Product Identifiers, and the agency evaluates submissions within a fixed 90-day timeframe.
- Use pre-submission meetings (EMA). The EMA actively encourages sponsors to engage before submitting. These meetings clarify documentation requirements and reduce the risk of rejection on procedural grounds.
Pro Tip: For the FDA application, resist the temptation to include exhaustive background literature. OOPD reviewers prioritize clarity. A well-organized 15-page submission with precise prevalence data and a clean scientific rationale consistently outperforms a 60-page document with buried key evidence.
The overcoming research barriers perspective matters here too. The application process itself is a strategic step, and treating it as documentation of your development thesis rather than a bureaucratic hurdle changes both the quality and the outcome.
FDA vs. EMA: key differences at a glance
Sponsors pursuing global development often apply for both FDA and EMA orphan designation, but the two programs require genuinely independent strategies. Here is a direct comparison:
| Feature | FDA (U.S.) | EMA (EU) |
|---|---|---|
| Prevalence threshold | Fewer than 200,000 U.S. patients | No more than 5 in 10,000 EU residents |
| Market exclusivity | 7 years post-approval | 10 years post-approval |
| Pediatric extension | Not applicable in same form | +2 years with compliant pediatric plan |
| Fee benefit | Full user fee waiver | Significant reductions; full waiver for SMEs |
| Pre-submission process | Optional meetings with OOPD | Strongly encouraged via IRIS platform |
| Application timing | Any stage before marketing approval | Any stage before marketing authorization |
| Scientific benefit requirement | Plausible connection to condition | Significant benefit over existing therapies required |
The EU's requirement for "significant benefit" sets a higher bar than the FDA's plausibility standard at the designation stage. Sponsors who have a treatment in a space with some existing options need to articulate a clear differentiation story for the EMA that the FDA does not explicitly require upfront.
Pursuing both designations makes strategic sense when a company targets global commercialization. The incentives do not overlap, so the combined package of 7-year U.S. exclusivity plus 10-year EU exclusivity, stacked with tax credits and fee waivers in both markets, can fundamentally change the financial model for a rare disease program.
Impact on treatment availability for rare disease patients
The orphan drug designation system has genuinely changed the rare disease landscape since 1983. FDA approvals for orphan drugs now comprise roughly one-third of all new drug approvals annually. That is a structural shift in pharmaceutical development priorities driven almost entirely by the incentive structure.
Yet the picture is incomplete without acknowledging the gaps. Consider these realities:
- Over 6,000 rare diseases are currently identified, but only about 10% have approved therapies despite more than 1,850 orphan designations granted by the FDA
- Oncology dominates the designation landscape, meaning rarer non-cancer diseases still receive disproportionately less attention
- Small patient populations make clinical trial recruitment extremely difficult, regardless of designation status
- Designation does not compel a sponsor to continue development; programs can be abandoned after designation is granted
The FDA approval pathways for orphan drugs have also created a pathway for personalized medicine approaches, with treatments like gene therapies increasingly using orphan status as an entry point into narrow genetic disease indications. That is a genuine win for patients with ultra-rare diseases.
The honest assessment is that orphan drug designation corrects a market failure but does not eliminate all barriers. It shifts the economics enough to attract development interest. Whether that interest translates to an approved, accessible therapy depends on clinical success, continued funding, and regulatory execution.
My perspective on what orphan designation really means
I have spent years watching families research orphan drug status for conditions affecting their children or loved ones, and the same misunderstanding surfaces consistently. They see a press release about a drug receiving FDA orphan designation and believe treatment is close. It is not, necessarily. Designation is a regulatory milestone, not a clinical one.
In my experience, the most valuable thing orphan designation does is create a structured argument for why a rare disease program deserves resources. It formalizes the unmet need, attaches financial incentives, and signals to investors and partners that regulators have acknowledged the space. That is genuinely meaningful, but it is a beginning, not an endpoint.
What I have seen go wrong most often is sponsors applying too late, after spending clinical trial resources that would have been partially covered by tax credits had they designated earlier. The second most common mistake is submitting a bloated application that obscures the key prevalence data. OOPD reviewers are not grading you on comprehensiveness. They want one number (how many patients?), one scientific argument (why would this work?), and clean documentation.
For patients and families, understanding orphan designation means knowing that when you see it attached to a drug targeting your condition, someone has made a formal commitment to develop that therapy and has received regulatory support to do so. That matters. But set expectations clearly. Designation is hope with infrastructure. It is not a cure on a timeline.
— John
How Hopeatrarelabs supports your rare disease research
If a drug targeting your rare disease has orphan designation, that is a starting point, not the full picture. Hopeatrarelabs exists precisely for the gap between "there is research" and "there is a treatment for my patient."

At Hopeatrarelabs, the team builds patient-specific disease models using iPSC technology and CRISPR gene editing to run parallel treatment screens across thousands of FDA-approved compounds. This means you are not waiting to see if an orphan-designated drug eventually reaches approval. You are actively searching for what might work now, using your patient's own biology. Visit the RareLabs knowledge hub to explore rare disease research and treatment data, or go directly to Hopeatrarelabs to start a personalized treatment search. For families who cannot afford to wait, this is where evidence-based urgency meets scientific rigor.
FAQ
What is the difference between orphan drug designation and approval?
Orphan drug designation is a regulatory status granted before approval that provides development incentives. Approval is the separate decision that allows a drug to be marketed and prescribed to patients.
How many patients qualify a disease for FDA orphan designation?
A disease must affect fewer than 200,000 people in the United States, a threshold established by the Orphan Drug Act of 1983.
Can a drug lose orphan drug status after it is designated?
Designation itself can be maintained, but orphan market exclusivity can be revoked after approval if the sponsor fails to demonstrate clinical superiority over a competing drug or cannot supply sufficient quantities to meet patient demand.
Should sponsors apply for both FDA and EMA orphan designation?
Yes, when targeting global markets. The two programs have independent application processes and non-overlapping incentives, so pursuing both maximizes market exclusivity and financial benefits across the U.S. and EU.
How do orphan drug incentives help patients with rare diseases?
By reducing financial risk for sponsors through tax credits, fee waivers, and market exclusivity, orphan drug incentives make it economically viable to develop treatments for diseases that would otherwise receive no pharmaceutical investment.